Print or print to save as PDF.
⚂ A.8.1 Overview.
⚂ A.8.2 Implications of neurodiversity for social sciences.
⚂ A.8.3 The TPD through a neurodiversity lens.
⚂ A.8.4 Is excitability related to autism?
⚂ A.8.5 4E cognition.
⚂ A.8.6 A bibliography on neurodiversity.
⚃ A.8.6.1 2024 Update: A bibliography on neurodiversity.
⚃ A.8.6.2 A bibliography on neurodiversity.
⚂ A.8.1 Overview.
I came up with the word “Neurodiversity” for two specific political functions 1. to add a necessary new category to what is now called “Intersectionality.” 2. to suggest an umbrella term for an emerging social/political movement based on the pioneering work of the Autistic Self-Advocacy Movement. It had become clear that ASA movement's paradigm was beginning to be adopted by other Neurotribes who had different diagnostic labels but common issues of exclusion. The intention was to sound authoritative based on the combined heft of neuroscience and environmental science, not to be scientific. Take Home Lesson: ND is not a classificatory term dividing us from them. We are all Neurodiverse. We live on a Neurodiverse planet in which amoral nature generates endless genetic diversity, while we humans have evolved the capacity to make judgments about nature’s bounty. What Neurodiversity brings us is a challenge to find a place for everyone and to distribute the bounty fairly (Singer, 2021, February 21).
⚃ This review is informative, and I do not express a stance on the topic.
⚃ Please be aware that there is currently ongoing debate and varying opinions regarding this topic.
⚃ Inspired by the idea of biodiversity, the term
‘neurodiversity’ was used in a book chapter published in 1999 by Judy Singer (Singer, 1999).
≻ The term also appeared in a magazine article written by Bloom (1998). Singer had suggested the term in their collaboration by email.
≻ Singer (2017) elaborated: “But the term ‘neurological diversity’ was too much of a mouthful to lend itself to sloganeering, until one day I found myself saying that what the world needed was a ‘Neurodiversity Movement.’ I wrote about it on InLv, mentioned it in my thesis, and in my essay, ‘Why can't you be normal for once in your life?”
≻ “I wanted to see a neurodiversity revolution as potent as the feminist revolution had been. I wanted to see if, given a more understanding, inclusive and supportive environment, whether a new type of human, capable of rising to a new level of human creativity, would evolve” (Singer, 2017).
⚃ Since its introduction, the term “neurodiversity” has been used in various ways by various stakeholders and the implicit context and meaning intended by the author is not always explained.
≻ No single definition has been accepted and used.
≻ Associated terms soon followed, for example: neurotype, neurotypical (see Arnold, 2017), neurominority (Walker), neuroqueer (Walker), neurodivergent (Asasumasu), and neurodivergence (Asasumasu).
⚃ Neurodiversity has
generally been associated with autism.
≻ As Singer (2017) said: “While my focus was on AS, I considered that the scope of neurodiversity was far broader. It could encompass the near-absurdist splinterings of the then DSM IV, even perhaps gender identity and sexual preference, surely properties of the mind.”
⚃ Many take neurodiversity to mean that autism should not be seen as a disorder or a pathology: it should be reconceptualized, as a normal variation in neurological functioning and accepted as such.
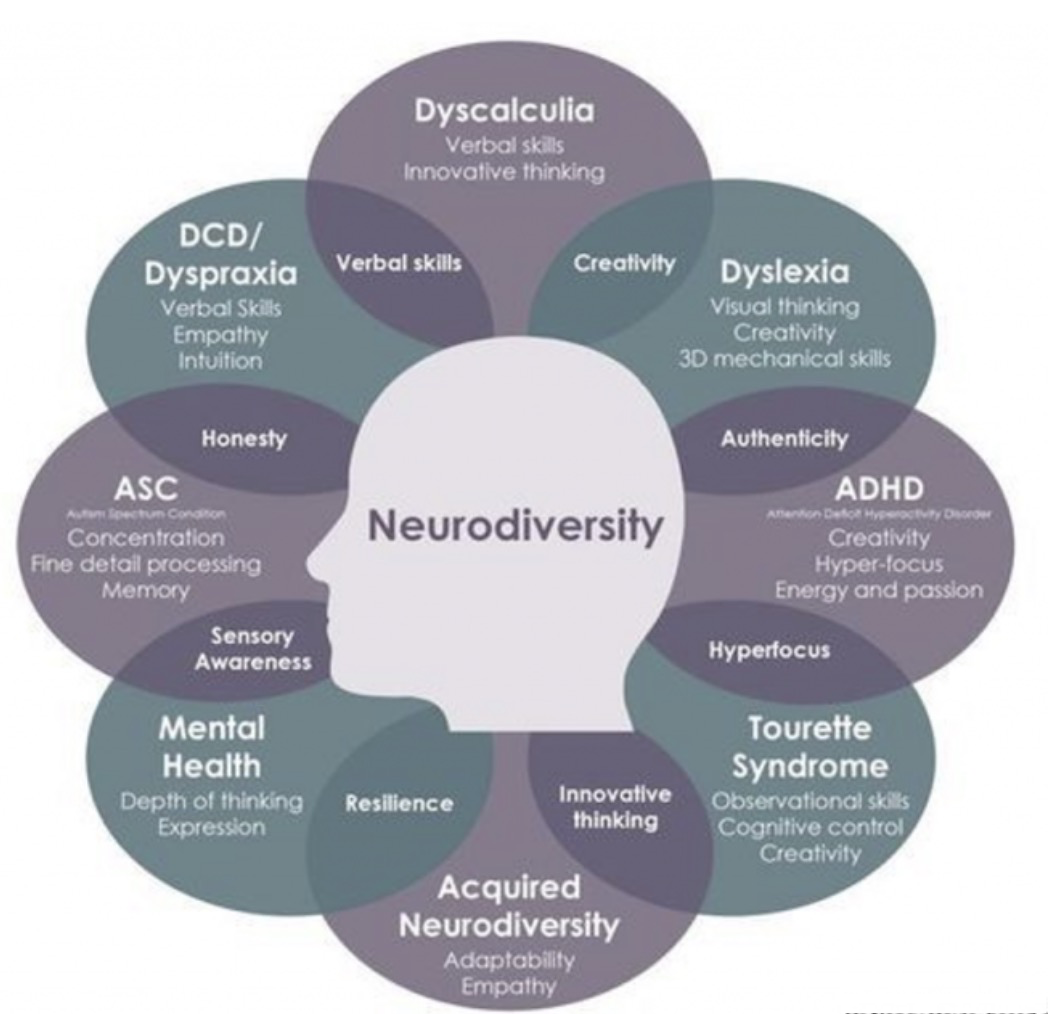
≻ Following this line of thought, today many authors extend neurodiversity to include dyspraxia, dyslexia, attention deficit hyperactivity disorder, dyscalculia, those with high sensitivity (Aron), synesthesia, and Tourette syndrome.
≻ Some authors include all mental health conditions, including those with physical basis, for example, MS and Parkinson’s.
≻ This perspective
generally rejects the medical model which sees disability as as a defect or impairment of an individual requiring treatment or cure.
≻ This new view is based upon the idea that divergent neurodevelopment should be seen as equivalent to typical neurodevelopment: that is to say it is not inferior to neurotypicality – neurodiversity does not differentiate “us from them” – every individual is neurodivergent.
≻ Another implicit assumption is that all individuals, either neurotypical or neurodivergent, deserve dignity, respect, and equality.
⚃ Some authors describe neurodiversity explicitly as a “movement” (or paradigm, approach, or framework).
≻ Walker (2021): (1) Neurodiversity is a natural and valuable form of human diversity,
≻ (2) The idea that there is one “normal” or “healthy” type of brain or mind, or one “right” style of neurocognitive functioning, is a culturally constructed fiction, and
≻ (3) The social dynamics that manifest in regard to neurodiversity are similar to the [social power inequalities] that manifest in regard to other forms of human diversity, [but] by which diversity, when embraced, acts as a source of creative potential.
≻ These dynamics include the dynamics of social power inequalities, and also the dynamics by which diversity, when embraced, acts as a source of creative potential.
≻ The Neurodiversity Movement is a social justice movement that seeks civil rights, equality, respect, and full societal inclusion for the neurodivergent.
⚃ García & Vázquez-del-Mercado, (2023, p. 3): “Indeed, most of the members of this movement claimed that referring to some cognitive and/or neural variations as 'impairments,' 'disabilities,' 'disorders,' etc. already had negative connotations that were exclusively socio-culturally induced – not induced by any condition found in the individual by herself – and were associated to forms of subjugation, abuse, and manipulation.”
⚃ Other points:
≻ In summary, some see autism as socially constructed and an imposed “disorder” that needs no cure and emphasize autism as a valuable minority identity.
≻≻ In this view, autistic people experience social impairments that call for social reforms – not medical interventions.
≻ Some see the neurodiversity movement as a civil rights movement.
≻ Some suggest that no research on autism be conducted without the direct involvement of autistic persons as stakeholders (“Nothing about us, without us”).
≻ Some presentations of neurodiversity and the neurodiversity movement are considered more radical than others.

⚃ Walker (2021) offers a detailed breakdown of the terminology:
≻ Neurodiversity is a biological fact.
≻≻ It’s not a perspective, an approach, a belief, a political position, or a paradigm.
≻≻ That’s the
neurodiversity paradigm;
≻ Neurodiversity is not a political or social activist movement.
≻≻ That’s the
neurodiversity movement, not neurodiversity itself.
≻ Neurodiversity is not a trait that any individual possesses or can possess; it’s used to describe a
group of people whose members differ neurocognitively from each other.
≻ An individual or group of individuals who diverge from the dominant societal standards of “normal” neurocognitive functioning are
neurodivergent.
≻ An individual cannot be neurodiverse [diverse = made up of multiple different types] – they are neurodivergent.
≻ Autism and dyslexia are forms of neurodivergence; any significant divergence from dominant cultural norms of neurocognitive functioning.
⚃ Definitions below are from:
https://exceptionalindividuals.com/neurodiversity/
≻
Neurodiversity – Noun: The diversity or variation of cognitive functioning in
groups of people.
≻≻ Neurodiversity is an approach [to education and ability] that supports the fact that various neurological conditions are the effect of normal changes and variations in the human genome.
≻
Neurodiverse – Adjective: Describes the diversity and variation of cognitive functioning in groups of people.
≻≻ Neurodiverse refers to a community of people whose members are neurodivergent.
≻
Neurodivergence – Noun: Cognitive functioning which is not considered “typical.”
≻≻ For example, autistic, dyslexic, and dyspraxic people.
≻≻ Every individual has a unique brain and therefore different skills, abilities, and needs.
≻
Neurodivergent – Adjective:
Describes an individual who has a neurodivergence.
≻ Neuro-differences are recognised and appreciated as a social category similar to differences in ethnicity, sexual orientation, gender, or ability.
≻ For example, a neurodivergent condition such as dyslexia is an integral part of a person.
≻ To take away their dyslexia is to take away from the person.
≻ It is common to mistakenly say neurodiverse when you mean neurodivergent.
≻
Summary: A group of people are neurodiverse, an individual is
neurodivergent.
⚃ For overview articles see: Dwyer, (2022) and Ne’eman and Pellicano, (2022).
≻ A seminal work on terminology is presented by Dr. Nick Walker, (2021).
⚂ A.8.2 Implications of neurodiversity for social sciences.
As Dwyer (2022) points out, neurodiversity is
generally presented as an alternative/replacement for the medical model.
≻ Here, I will review the medical and social models and present Dwyer's (2022) suggestion for a middle-of-the-road approach.
⚃ A.8.2.1 The medical model of disability.
The medical model emphasizes a deficiency, disease or abnormality in the bodily functions of an individual.
≻ Health is the absence of disease or abnormality.
≻ The individual is the locus of intervention aimed at fixing and ameliorating the problem to return to a state of health – normality.
≻ In this approach the expert is considered the authority and the social context remains static.
≻ The roots of this approach are usually traced to Louis Pasteur’s germ theory according to which germs infect organs from the outside and thus cause disease (Gobo, Campo, & Portalupi, 2023; Haegele, & Hodge, 2016).
The origin of the medical model is often attributed to R. D. Laing.
≻ In 1969, R. D. Laing introduced the term “the medical model” to broadly refer to the training of doctors and the practice of medicine.
≻ It’s worthwhile to quote Laing at some length because his work is seminal and establishes a historical context.
Medical diagnosis finds its place in the context of a set of procedures in which all doctors are trained and which influences for life all who have been trained in them. Essentially it is this. When one comes to see anyone as a patient, one listens to the complaint, cakes a history, does an examination, institutes whatever supplementary investigations one feels to be necessary, arrives at a diagnosis, makes a prognosis if one can, and having done all that, one prescribes treatment. Complaint, history, examination plus investigations, diagnosis, prognosis, treatment. Diagnosis includes aetiology, where aetiology is thought to be known. Often it implies prognosis. In all cases it determines treatment: no rational therapy without prior diagnosis: it is reckless and irresponsible to attempt to treat anyone without having arrived at, at least, a tentative diagnosis on the basis of which one's treatment is instituted” (Laing, 1969/1972, p. 39).
Laing goes on to differentiate medical versus social models.
One encounters a situation, defined in the first place by the people in it, and/or by agents in other situations. As soon as one is presented with any situation one is interacting with elements of it, and hence, willy-nilly intervening in one way or another. As soon as one intervenes, the situation changes somewhat, however little. A doctor does not usually feel he intervenes, in this sense, in the processes of, say, cardiovascular failure, or tuberculosis, simply by hearing the complaint, taking a history, doing an examination. He has not started to intervene with a view to change until he begins his treatment, after he has done all that is necessary to arrive at his diagnosis. In our case, we are intervening in and changing the situation as soon as we are involved. As soon as we interplay with the situation, we have already begun to intervene willy-nilly. Moreover, our intervention is already beginning to change us, as well as the situation. A reciprocal relationship has begun. The doctor and the still predominantly medically oriented psychiatrist use a non-reciprocal static model: history comes after the complaint; examination comes after the history; after this one makes a tentative or if possible definitive diagnosis; thereafter comes 'therapy.' Diagnosis is dia: through; gnosis: knowledge of. Diagnosis is appropriate for social situations, if one understands it as seeing through the social scene. Diagnosis begins as soon as one encounters a particular situation, and never ends. The way one sees through the situation changes the situation” (Laing, 1969/1972, pp. 39-40).
Laing draws contrasts between the two models but does not seem to describe them as diametrically opposed: rather, they are interrelated and it seems elements of both are required.
≻ We quote Laing again extensively because he explicitly explains the relationship between the two models.
Social diagnosis is a process: not a single moment. It is not an element in an ordered set of before after events in time. In the medical model, such a sequence is the ideal, to which one tries to approximate in practice: complaint; history; examination; diagnosis; treatment. Intervention in social situations may have different phases: they overlap, contrapuntally. The phases cannot be chopped up into time-slices. What one sees as one looks into the situation changes as one hears the story. In a year's time, after one has got to know the people and their situation a little, the story will have gone through a number of transformations: often it will be very different from what one heard a year back; neither version is necessarily untrue or true. It is a different story, or one hears a different story. As the story is transformed as time goes by, so what one sees undergoes transformations. At a particular time one is inclined to define the situation in a particular way; this definition in turn changes the situation in ways we may never be able to define. One's definition of the situation may generate different stories. People remember different things, put things together in different ways. This redefines the situation as changed by our definition in the light of how it originally presented itself to us. Our definition is an act of intervention that changes the situation, which thus requires redefining; it introduces a new factor. At any moment of time, in the continuous process of looking through, of diagnosis, we see it in a particular way that leads us to a nondefinitive definition, subject to revision in the light of the transformations that this very definition induces, prospectively and retrospectively. Medically, our diagnosis does not affect the fact that the person has tuberculosis. We do not change the illness by our diagnosis. You do not convert a case of tuberculosis into a cardiac failure by calling it cardiac failure. But suppose our diagnosis of a situation is: This is a social crisis, due to the fact that this boy has 'got schizophrenia. We must treat the 'schizophrenia' in the boy, and the social worker must help the relatives to cope with the terrible tragedy of having a mental illness in the family and so forth. This is not merely a medical diagnosis. It is a social prescription. As you know, in my view, it is a gross misreading of the situation. In any event, whether you agree with me or not, there is no doubt that any such medical diagnosis also defines and changes the situation. Such a definition may even be an 'aetiological factor' in creating the situation one has defined: even in creating the 'illness' one is purporting to cure. Social situations are the field for the self-fulfilling prophecy. A self-fulfilling diagnosis of the situation tends to induce a situation as defined. One must not be naive. Who are the experts in such matters? Not many psychiatrists at present. Most have no training whatever in this respect, and have often been trained to be incompetent in this regard. We all must continually learn to unlearn much that we have learned, and learn to learn that we have not been taught. Only thus do we and our subject grow” (Laing, 1969/1972, pp. 40-42).
⚃ A.8.2.2 The social model of disability.
There are many different variations of the social model and little agreement on a single approach.
≻ In simple terms, the model shifts the focus of disability, disease, or impairment from the individual to their broader social environment.
≻ A “strong” version of the model rejects the medical model and sees society as the root cause of an individual’s disability.
≻ “The concept is almost invariably illustrated with architectural barriers faced by wheelchair users.
≻≻ It is one thing to be unable to walk.
≻≻ It is quite another matter to be unable to enter a building unassisted because the architect preferred stairs to ramps” (Samaha, 2007, pp. 1258-59).
“Those who accept this model assert that all (or most) so-called 'disorders' listed in the standard manuals basically are social constructs; they are neither pathological nor abnormal.
≻ Indeed, the very labels 'disorders,' 'pathologies,' 'abnormal,' 'divergent phenotypes,' 'deficits,' 'anomalies,' and so on, are all a part of this exclusionary social artifact that reinforces the denial of rights and opportunities to many people who are
simply different in some cognitive, neural and/or behavioral respects.” (García & Vázquez-del-Mercado, 2023, p. 4).
Generally, the model differentiates between personal impairment and disability.
≻ Disability is bifurcated into “(1) personal impairment and (2) a social setting comprising architecture, economics, politics, culture, social norms, aesthetic values, and assumptions about ability” (Samaha, 2007, p. 1257).
≻ In this way, disability is imposed on individuals by their social environments.
≻≻ The emphasis is on the environment.
≻ Thus, the individual’s impairment is not the root cause of any subsequent disability.
≻ Following this thinking, intervention is not aimed at the individual; it is directed at adapting and improving the individual’s social environment.
In summary, in the social model, disability arises from an environment that does not accommodate an individual’s unique characteristics.
≻ Interventions must be social and political to both adapt the physical environment and to create understanding and welcoming social networks that emphasize social inclusion of all.
≻ Society thus evolves to be more understanding and inclusive, accepting the uniqueness of all individuals.
≻ Those who are disabled become the experts and advocates whose role it is to advise and evoke change.
⚃ A.8.2.3 A contemporary way forward.
Today, proponents of both the neurodiversity and the social models present them as an alternative to the medical model (Dwyer, 2022).
≻ On the other hand, Singer (2017) suggested that neurodiversity be a middle ground between the medical and social models (Dwyer, 2022).
≻ Dwyer (2022, p. 76) advocates this unifying presentation of neurodiversity, observing that “It is not difficult to think of cases wherein characteristics of both the individual and their environment contribute towards disability.”
Dwyer (2022, p. 86) concludes: “Although the neurodiversity approaches are evolving and although their relation to the social model of disability remains a subject of debate, it is here proposed that the optimal neurodiversity approach should take a middle ground between the social and medical models, as suggested by Singer (2016).
≻ This neurodiversity approach would consider disability as emerging from an interaction of individual and context, and it would allow interventions to either change individuals in limited ways (e.g., teaching skills, using medication to manage difficulties) or to change environments and societies.”
Laing’s approach, presented above, seems eerily prescient of the relationship described between the medical and social models in Dwyer’s (2022) “middle ground approach” to neurodiversity.
Here is a summary of Dwyer’s (2022) “middle ground approach.”
≻ Disability arises from an interaction between the characteristics of the disabled individual and their environment.
≻ Disability can be addressed either by addressing the environment (e.g., reshaping environments and societal attitudes toward disability) and/or by changing the individual.
≻ To cure or normalize disabled individuals should not be the goal.
≻ Diversity should be valued without judgement and individuals with neurological disabilities should be accepted for who they are.
⚂ A.8.3 The TPD through a neurodiversity lens.
⚃ Dabrowski’s theory of positive disintegration emphasizes development is predicated upon the amount and valence of the genetically based characteristics linked to development: the developmental potential.
≻ These elements, including instincts, dynamisms, special abilities and talents, overexcitability, and the third factor are critical characteristics of the individual that determine the parameters of their potential development.
≻ Expressed through the dynamisms and third factor, the individual plays a critical role in promoting and directing their own development.
≻ The individual constructs a hierarchy of values and personality ideal that come to direct their pursuit of a unique and authentic personality.
⚃ Dabrowski also considers the role of the environment.
≻ The environment is less important when the individual’s potential is positive and strong but becomes paramount when the strength or valence of the developmental potential is equivocal.
≻ In these cases, a positive environment is required for growth, and a negative environment usually thwarts development.
⚃ Individuals who display developmental potential could be seen as having a neurotype, as these characteristics only occur in a minority of people.
≻ Dabrowski’s theory could be seen in the context of the “middle ground approach” to neurodiversity suggested by Dwyer (2022).
⚂ A.8.4 Is excitability related to autism?
⚃ A major theory of the etiology of autism is a disruption of the excitatory and inhibitory balance. Here are a few salient references.
⚃ Bruining, H., Hardstone, R., Juarez-Martinez, E. L., Sprengers, J., Avramiea, A. E., Simpraga, S., Houtman, S. J., Poil, S. S., Dallares, E., Palva, S., Oranje, B., Matias Palva, J., Mansvelder, H. D., & Linkenkaer-Hansen, K. (2020). Measurement of excitation-inhibition ratio in autism spectrum disorder using critical brain dynamics.
Scientific Reports, 10 (1), 9195.
https://doi.org/10.1038/s41598-020-65500-4
≻ Excitatory (E) and inhibitory (I) systems are critical for regulating the flow of information in the brain.
≻ Without narrow control over the E/I ratio, runaway excitation or quiescence would occur, impeding adequate information processing.
≻ In clinical terms, disruption of E/I balance has become a dominant theory on the pathogenesis of various neurodevelopmental disorders, and perhaps most explicitly in autism spectrum disorder (ASD).
≻ We have introduced a measure of functional E/I ratio (fE/I) from network activity that is sensitive to both changes in synaptic functioning and network connectivity and which is applicable to non-invasive human EEG recordings
≻ In spite of the comprehensive literature on E/I balance, there is no consensus on how to define or measure E/I ratio, neither functionally or structurally.
≻ The design of our measure of fE/I was guided by the theory of critical brain dynamics, which is rooted in the physics concept of critical phase transitions
≻ In conclusion, we propose that parallel quantification of the critical brain dynamics indices of power, LRTC and fE/I may provide a novel theory-based framework to advance understanding of physiological heterogeneity of ASD and related disorders.
⚃ Culotta, L., & Penzes, P. (2020). Exploring the mechanisms underlying excitation/inhibition imbalance in human iPSC-derived models of ASD.
Molecular Autism, 11 (1), 32.
https://doi.org/10.1186/s13229-020-00339-0.
≻ One of the proposed etiological mechanisms of ASD is the disruption of the balance between excitation and inhibition (E/I balance) in key cortical and subcortical neuronal circuits
≻ In this review, we will focus on human iPSC-derived in vitro models of ASD and summarize the most recent studies in which the iPSC technology has been exploited to investigate the molecular bases of E/I imbalance and to gain further insight into the etiological mechanisms of ASD
≻ The complex genetic etiologies and clinical phenotypes observed in ASD patients hinder the research of the pathophysiological mechanisms underpinning ASD and the quest for pharmacological treatments.
≻ In particular, a growing body of literature has provided evidence of altered balance between excitation and inhibition in human-based models of ASD.
≻ These have been linked to disruptions in different neuronal mechanisms contributing to the generation and regulation of E/I balance, such as homeostatic plasticity, synaptic transmission, and neuronal excitability.
≻ Furthermore, the recent advent of brain organoids has represented a great advance in modeling of ASD, providing a more valuable model of brain development in which to assess E/I imbalance.
≻ Indeed, organoids recapitulate several morphological and functional features of the developing human brain, and have the potential to be a more predictive drug screening platform.
≻ These advances support the study of iPSC-derived neuronal systems as key in unlocking pathogenic mechanisms and potential treatment avenues in ASD.
⚃ Foss-Feig, J. H., Adkinson, B. D., Ji, J. L., Yang, G., Srihari, V. H., McPartland, J. C., Krystal, J. H., Murray, J. D., & Anticevic, A. (2017). Searching for cross-diagnostic convergence: Neural mechanisms governing excitation and inhibition balance in schizophrenia and autism spectrum disorders.
Biological Psychiatry, 81 (10), 848–861.
https://doi.org/10.1016/j.biopsych.2017.03.005
≻ In this article, we take a clinical neuroscience perspective, highlighting emerging evidence from human neuroimaging studies testing markers of E/I imbalance in cortical microcircuits.
≻ Though no studies have examined E/I balance cross diagnostically, we evaluate evidence from parallel ASD and SCZ literatures in considering shared and divergent pathways.
≻ We discuss the problem whereby E/I imbalance becomes yet another overly general hypothesis, with minimal mechanistic precision or predictive power, for explaining diverse symptomatology (Supplement).
≻ To address this challenge, we highlight where E/I imbalance contributes to specific symptoms that may be constrained developmentally or neuroanatomically.
≻ Finally, we argue that refining the E/I imbalance hypothesis should occur cross-diagnostically with an ultimate goal of informing novel treatments targeting related pathways across neurodevelopmental disorders.
≻ Despite a clear need for translational research to further dissect the nature and extent of E/I imbalance across ASD and SCZ, some consistent themes emerged across this complex neuroimaging literature (e.g., progressive effects in SCZ apparent in both 1 H-MRS and rs-fMRI studies).
≻ Additionally, correlations between neural metrics of E/I imbalance and symptom levels were often reported. This pattern suggests that the magnitude of E/I imbalance may relate to clinical severity in a graded manner.
≻ Differences observed over the course of illness in SCZ and between children and adults with ASD point to the importance of understanding whether E/I alterations are temporally stable or fluctuate over development.
⚃ Karjalainen, S., Aro, T., & Parviainen, T. (2023). Coactivation of autonomic and central nervous systems during processing of socially relevant information in autism spectrum disorder: A systematic review.
Neuropsychology Review.
https://doi.org/10.1007/s11065-023-09579-2
≻ The results indicated that individuals with ASD demonstrate atypicalities in ANS and CNS signalling which, however, are context dependent.
≻ There were also indications for altered contribution of ANS-CNS interaction in processing of social information in ASD.
≻ However, the findings must be considered in the context of several limitations, such as small sample sizes and high variability in (neuro) physiological measures.
≻ Indeed, the methodological choices varied considerably, calling for a need for unified guidelines to improve the interpretability of results.
≻ We summarize the current experimentally supported understanding of the role of socially relevant body-brain interaction in ASD.
≻ Furthermore, we propose developments for future studies to improve incremental knowledge building across studies of ANS-CNS interaction involving individuals with ASD.
≻ The aim of this article was to systematically review and qualitatively synthesize the empirical evidence regarding differences in ANS and CNS activation as well as body-brain interaction during social information processing between individuals with ASD and typically developing individuals.
≻ The focus was on studies where both ANS and CNS activity were simultaneously measured.
≻ In summary, the results of this systematic review demonstrate coexisting but context dependent ANS and CNS atypicalities during processing of socially relevant information among individuals with ASD.
≻ Furthermore, there is indication of altered reactivity and/or trait features in ANS activity among individuals with ASD that may contribute to social information processing by influencing the perception and processing of socially relevant stimuli in the brain.
⚃ Lee, E., Lee, J., & Kim, E. (2016). Excitation/inhibition imbalance in animal models of autism spectrum disorders.
Biological Psychiatry, 81 (10), 1–10.
https://doi.org/10.1016/j.biopsych.2016.05.011.
≻ This review summarizes results from animal models of ASD showing altered E/I balances.
≻ E/I balance is established and tightly regulated by a large number of factors, making it difficult to differentiate primary changes from secondary alterations in model animals, as was recently noted.
≻ These results collectively suggest that an increased neocortical E/I ratio caused by malfunctions of PV-expressing interneurons induces excessive gamma oscillations and autistic-like behaviors.
≻ Pathogenic mechanisms underlying E/I imbalance in ASDs are more complex than might have been expected.
≻ Recent studies have even begun to show that the same gene mutation leads to distinct synaptic E/I imbalances in different synapses, cell types, and brain regions at different time points.
≻ Collectively, these findings highlight the importance of pursuing detailed and integrative analyses of E/I imbalances in future studies of animal models of ASD.
⚃ LeMieux, J. (2020, August 5). Autistic men have enhanced excitability in social brain regions. GEN – Genetic Engineering and Biotechnology News. https://www.genengnews.com/news/autistic-men-have-enhanced-excitability-in-social-brain-regions/ A description of the study by Trakoshis et al, (2020).
⚃ Manyukhina, V. O., Prokofyev, A. O., Galuta, I. A., Goiaeva, D. E., Obukhova, T. S., Schneiderman, J. F., Altukhov, D. I., Stroganova, T. A., & Orekhova, E. V. (2022). Globally elevated excitation–inhibition ratio in children with autism spectrum disorder and below-average intelligence.
Molecular Autism, 13 (1), 20.
https://doi.org/10.1186/s13229-022-00498-2.
≻ Although Rubenstein and Merzenich initially related ASD to an elevated E–I ratio, later it became clear that some forms of ASD can be characterized by decreased E–I ratio and that alternations in the E–I ratio can be region-specific, reflecting homeostatic regulation of local E–I imbalances.
≻ Still, there is evidence that, in many cases, the global deficit associated with ASD can be characterized as predominant neuronal hyper- or hypo -excitability.
≻ Therefore, despite simplification, the concept of a global E–I balance is important for understanding the pathophysiological mechanisms associated with ASD.
≻ Here, we used MEG and individual magnetic resonance imaging (MRI)-based brain models to capture the spectral slope from high-frequency brain activity measured ‘at rest’ in children with ASD and below-average IQ, those with average IQ, and in age-matched TD children.
≻ There is strong evidence that brain structure and functioning, including the E–I balance, may be differently affected in males and females with ASD.
≻ In conclusion, the abnormally flattened 1/f spectral slope estimated in the high-frequency part of the MEGdetected neural activity spectrum is likely to reflect neuronal E–I imbalance associated with intellectual disability in children with ASD.
≻ Participants with below-average IQ are heavily underrepresented in autism research and most neuroimaging studies only include high-functioning individuals with ASD.
≻ Our MEG study demonstrates that it is feasible to collect resting-state MEG and structural MRI data in children with below-average IQ, and that cognitive ability, even though it is not a core aspect of the ASD diagnosis per se, should be considered as an important factor for research in the pathophysiology of this neurodevelopmental disorder.
≻ Our results indicate that the 1/f spectral slope estimated in the high-frequency part of the neural activity power spectrum may be a useful and objective biomarker of changes to the E–I ratio induced by pharmacological and other therapeutic interventions in low-functioning children with ASD.
⚃ Pressey, J. C., de Saint-Rome, M., Raveendran, V. A., & Woodin, M. A. (2023). Chloride transporters controlling neuronal excitability.
Physiological Reviews, 103 (2), 1095-1135.
https://doi.org/10.1152/physrev.00025.2021
≻ Numerous neurodevelopmental, neuropsychiatric, and neurological disorders result from the dysfunction of cI- transporters, which alters the strength of synaptic inhibition.
≻ A decrease in, or dysfunction of, the neuron-specific ci--extruding transporter KCC2 contributes to seizure generation, neuropathic pain, and autism spectrum disorders (ASDs).
≻ Inhibition of the cI- importing transporter NKCC1, to reduce the concentration of intracellular cI-, has been a successful strategy to rescue synaptic inhibition and improve neuronal circuit function and behavioral outcomes in animal models of neurological disorders resulting from KCC2 dysfunction.
≻ The development of 1) next-generation cI- imaging tools, 2) next-generation NKCC1 inhibitors, and 3) a KCC2 enhancer/activator toolkit will facilitate a dramatic increase in both our understanding of CCC function and our ability to treat neurological disorders with underlying CCC dysfunction.
⚃ Rubenstein, J. L. R., & Merzenich, M. M. (2003). Increased ratio of excitation/inhibition in key neural systems: Model of autism.
Genes, Brain and Behavior, 2 (5), 255–267.
https://doi.org/10.1034/j.1601-183X.2003.00037.x
≻ In the following sections, we have attempted to initiate the dissection of mechanisms that may underlie some forms of autism.
≻ We begin by considering some aspects of the neural systems that could play central roles in behaviors that are disrupted in autism.
≻ The existing evidence discussed above suggests the following characteristics of the genetic contribution to autism:
≻ 1. Multiple genes can cause autism alone or in combination with other genes.
≻ 2. No one gene is necessarily a major determinant of autism.
≻ 3. Genes that cause autism may not do so in all people carrying the same mutation.
≻ Differential penetrance may occur if the individual: (i) hasn’t co-inherited other susceptibility genes; (ii) hasn’t been exposed to the same environmental insults; (iii) if there is a stochastic contribution to a relevant developmental process.
≻ If autism is caused by an increase in the ratio of excitation/inhibition in one of several key neural systems, then autism could be caused by co-inheritance of alleles that either increase excitation or reduce inhibition in these neural systems.
≻ Thus while inheriting one allele which reduces inhibitory signaling (or increases excitatory signaling) in the cortex may not result in a noticeable pathophysiology, coinheritance of two or more such alleles, that further increase the excitation/inhibition ratio, perhaps in conjunction with environmental factors that likewise affect neural signaling, would increase the probability of neural dysfunction.
≻ In summary, increasing the ratio of excitation/inhibition in key neural systems, either genetically or epigenetically, is postulated to be the common pathway for causing autism.
≻ This hypothesis can be useful for considering the genetic and epigenetic mechanisms that contribute to autism, for generating animal models that may mimic aspects this disorder and for considering potential therapies.
⚃ Takarae, Y., & Sweeney, J. (2017). Neural hyperexcitability in autism spectrum disorders.
Brain Sciences, 7 (10), 129–129.
https://doi.org/10.3390/brainsci7100129
≻ While the model of cortical excitability has gained widespread support from genetic and epigenetic studies, its specific effects on observed behavioral phenotypes in ASD are not well established.
≻ This review will use examples of sensory processing abnormalities to illustrate how cortical excitability can influence neuronal processes eventually to affect behavioral phenotypes.
≻ Elevation in cortical excitability is observed in ASD at genetic, epigenetic, neural, and behavioral levels.
≻ While changes in cortical excitability affect general cognitive function, cortical excitability has especially profound effects on sensory phenotypes in ASD.
≻ The effect on sensory phenotypes is complex, affecting sensory processes through multiple different neural processes, which may contribute to the heterogeneous expression of symptoms.

⚃ Trakoshis, S., Martínez-Cañada, P., Rocchi, F., Canella, C., You, W., Chakrabarti, B., Ruigrok, A. N., Bullmore, E. T., Suckling, J., Markicevic, M., Zerbi, V., MRC AIMS Consortium, Baron-Cohen, S., Gozzi, A., Lai, M. C., Panzeri, S., & Lombardo, M. V. (2020). Intrinsic excitation-inhibition imbalance affects medial prefrontal cortex differently in autistic men versus women.
ELife, 9, e55684.
https://doi.org/10.7554/eLife.55684
≻ While no one theory can fully explain all individuals with an autism diagnosis, the E:I imbalance theory may have utility for understanding subtypes of autistic individuals.
≻ In conclusion, we show that spectral properties of neural time-series data, such as H [H = Hurst exponent is used as a measure of long-term memory of time series] and 1/f slope, can be utilized in neuroimaging readouts like LFP and BOLD as a biomarker for underlying E: I-relevant mechanisms. finally, in application to humans, we show that H in rsfMRI data is reduced in vMPFC and other DMN areas of adult autistic males, but not females.
≻ Reduced H is indicative of enhanced excitation and thus points to sex-specific dysregulation of E:I balance in social brain networks of autistic males.
≻ This male-specific dysregulation of E:I balance may be linked to sex-differential early developmental events such as androgen-upregulation of gene expression for genes that play important roles in excitatory neurons.
≻ The intact levels of H in females may help facilitate elevated levels of compensation known as camouflaging to cope with daily social-communicative difficulties.
≻ This important female-specific brain-behavioral correlation may also be key for future interventions targeting E:I mechanisms and MPFC-related brain networks to enable better coping with daily social-communicative difficulties.
⚃ Zhang, P., Omanska, A., Ander, B. P., Gandal, M. J., Stamova, B., & Schumann, C. M. (2023). Neuron-specific transcriptomic signatures indicate neuroinflammation and altered neuronal activity in ASD temporal cortex.
Proceedings of the National Academy of Sciences, 120 (10), e2206758120.
https://doi.org/10.1073/pnas.2206758120.
2206758120
≻ This study aimed to identify neuron-specific transcriptomic changes in ASD brain by identifying differentially expressed genes, differential splicing (DS) events, age-related gene expression changes across the lifespan, and co-expression networks to reveal gene modules altered in ASD.
≻ In summary, our age-related findings support the premise brain development in individuals with ASD deviates from that of the neurotypical trajectory beginning in childhood and continues to evolve across the lifespan.
≻ Although the STG remains relatively unexplored, other brain regions display early excess followed by reductions in volume, connectivity, and cell densities as people with ASD age through adulthood.
≻ Initial excess and overconnectivity may lead to hyperexcitation, rendering the brain vulnerable to age-related and pro-inflammatory mechanisms contributing to later degenerative outcomes.
≻ Our findings of altered neuroinflammatory expression patterns, taken together with reports of excessive microglial activation in STG, implicate immune dysfunction in the pathophysiology of ASD that may exacerbate with age.
≻ Additionally, we found significant relationships with our ASD transcriptome profiles and AD profiles in the same brain region, supporting recent theories of increased susceptibility to neurodegenerative and cognitive decline.
≻ Lastly, our findings of an age-related decrease in GAD expression in bulk STG tissue, and an overall downregulation of GAD in neurons, further supports the hypothesis that GABAergic inhibitory neurons are disproportionally affected in ASD throughout the lifespan.
⚂ A.8.5 4E cognition.
⚃ “By using the term
embodied we mean to highlight two points: first, that cognition depends upon the kinds of experience that come from having a body with various sensorimotor capacities, and second, that these individual sensorimotor capacities are themselves embedded in a more encompassing biological, psychological, and cultural context.
≻ By using the term
action we mean to emphasize once again that sensory and motor processes, perception and action, are fundamentally inseparable in lived cognition. Indeed, the two are not merely contingently linked in individuals; they have also evolved together.
≻ We can now give a preliminary formulation of what we mean by enaction. In a nutshell, the
enactive approach consists of two points:
≻ (1) perception consists in perceptually guided action and
≻ (2) cognitive structures emerge from the recurrent sensorimotor patterns that enable action to be perceptually guided.
≻ These two statements will perhaps appear somewhat opaque, but their meaning will become more transparent as we proceed” (Varela, Thompson, & Rosch, 1991/2016, p. 173).
⚃ “ I turn to the ever-growing field of
embodied embedded extended and
enactive cognition, also referred to as
4E cognition. 4E cognition harbors a variety of subtly different takes on the view that cognition is the activity of a living
embodied embedded organism, whose cognitive apparatus
extends into and is shaped by its material and social environment and who has a stake in the world whose meaning it helps
enact (Clark 2008; Colombetti 2014; Gallagher 2005; Noë 2004; Rietveld 2008; Thompson 2007).
≻ In line with the phenomenological tradition they are indebted to, many 4E thinkers have focused their efforts not only on offering accounts of typically developed (human) cognition, but also on (re)describing and explaining cognitive 'disorders' such as autism.
≻ 4E proposals that have rejected ToMD and opened up new ways of understanding and explaining the cognitive, affective, experiential and behavioral dimensions of autism, particularly as they pertain to social cognition, have been offered by Fuchs (2015), Gallagher (2004 & 2008), Hutto (2003), De Jaegher (2013), Krueger & Maiese (2018) and Zahavi & Parnas (2003), just to name a few” (van Grunsven, 2020, p. 3).
⚃ “ 4E approaches to autism and social cognition can accommodate the idea of neurodiversity, where, to repeat, the idea of neurodiversity proposes to understand autism (and perhaps other 'disorders' such as ADHD, dyslexia, and Tourette Syndrome) not as a deficiency but as a cognitive variation in human mindedness that can be considered valuable both to the autistic individual herself and society at large” (van Grunsven, 2020, p. 3).
⚄ A.8.6.1 2024 Update: A bibliography on neurodiversity.
⚅ Axbey, H., Beckmann, N., Fletcher-Watson, S., Tullo, A., & Crompton, C. J. (2023). Innovation through neurodiversity: Diversity is beneficial. Autism, 27(7), 2193-2198. https://doi.org/10.1177/13623613231158685
≻ Neurodivergences such as autism have been previously viewed from a negative, ‘deficit,’ perspective.
≻ However, research is beginning to show the benefits of being autistic, and the positive outcomes of neurodiverse interactions.
≻ Diversity in the way we think can lead to diversity in the outcomes we produce.
≻ In this study, we asked independent raters to compare the similarity of towers built by autistic and non-autistic individuals in single-neurotype (both people were autistic or both people were non-autistic) and neurodiverse (one autistic person and one non-autistic person) pairs, to see whether people would be more or less likely to copy someone who shared their diagnostic status.
≻ Our results showed there was the least similarity in design in the neurodiverse pairs; people were less likely to copy the design of the previous builder if that person had a different autistic status to themselves.
≻ This could imply people felt more confident in copying someone with a similar neurotype, mirroring results from rapport studies where autistic individuals reported greater rapport with other autistic participants than with non-autistic participants.
≻ This also shows there was more evidence of creativity in designs, and innovation from stimulus design (the tower they had watched being built) when the pairs had different autistic diagnoses.
≻ This could inform practice and support involving autistic people, encouraging education and care providers to create more diverse methods and designs for support mechanisms, content delivery, and research data collection.
⚅ Barnett, J. P. (2024). Neuroqueer frontiers: Neurodiversity, gender, and the (a)social self. Sociology Compass, 18(6), e13234. https://doi.org/10.1111/soc4.13234
≻ This paper critically synthesizes leading edge scholarship on neurodiversity, arguing that sociology could expand its account for the relationship between self and society through attention to the (a)social practices of those constructed as neurologically disabled.
≻ Autistic scholaractivism birthed the neurodiversity paradigm, which claims respect for neurological diversity and its social manifestations.
≻ Sexual and gender variation are among those.
≻ I review research on the confluence of neurological, sexual, and gender variance, pointing to opportunities for documenting the roles of social institutions in constructing and regulating divergent bodyminds, as well as new intersectional identities and social movements.
≻ Next, I synthesize nascent literature developing neuroqueer theory.
≻ “Neuroqueer” articulates the queer nature of neurodivergence and examines the entwinement of the two.
≻ Centering the epistemic authority of bodyminds problematized as lacking self-control/intent, perspective-taking, and reliance on the social symbolic, neuroqueer scholars forward (a)social ways of knowing, communicating, communing, and being human.
≻ Focusing on neuronormativity, interdependent with better-recognized normativities (e.g., gender, ethnicity, etc.), neuroqueer theory offers fresh perspective on how dominant concepts and relations render some bodyminds problematic—legitimate objects of exclusion, marginalization, and “rehabilitation.”
≻ In doing so, it troubles sociological ideas about agency, sociality, communication, and what it means to be/have a (social) self.
⚅ Botha, M., Chapman, R., Giwa Onaiwu, M., Kapp, S. K., Stannard Ashley, A., & Walker, N. (2024). The neurodiversity concept was developed collectively: An overdue correction on the origins of neurodiversity theory. Autism, 28(6), 1591-1594. https://doi.org/10.1177/13623613241237871
≻ We, an international group of autistic scholars of autism and neurodiversity, discuss recent findings on the origins of the concept and theorising of neurodiversity.
≻ For some time, the coinage and theorising of the concept of ‘neurodiversity’ has been attributed to Judy Singer.
≻ Singer wrote an Honours thesis on the subject in 1998, focused on autistic activists and allies in the autistic community email list Independent Living (InLv).
≻ This was revised into a briefer book chapter, published in 1999.
≻ Despite the widespread attribution to Singer, the terms ‘neurological diversity’ and ‘neurodiversity
≻were first printed in 1997 and 1998, respectively, in the work of the journalist Harvey Blume, who himself attributed them not to Singer but rather to the online community of autistic people, such as the ‘Institute for the Study of the Neurologically Typical.’
≻ Recently, Martijn Dekker reported a 1996 discussion in which one InLv poster, Tony Langdon, writes of the ‘neurological diversity of people. i.e. the atypical among a society provide the different perspectives needed to generate new ideas and advances, whether they be technological, cultural, artistic or otherwise.’
≻ Going forward, we should recognise the multiple, collective origins of the neurodiversity concept rather than attributing it to any single author.
⚅ Chapman, R. (2023). Neurodiversity, Anti-Psychiatry, and the Politics of Mental Health. In S. Tremain (Ed.). The Bloomsbury guide to philosophy of disability (pp. 117-135). London: Bloomsbury Academic. http://dx.doi.org/10.5040/9781350268937.0011
≻ An examination of the meaning and significance of the neurodiversity movement must, at its outset, take into consideration that there is no leader of the movement, nor is it grounded in a foundational textbook or other official founding document.
≻ Nevertheless, the claims of certain influential theorists and activists, as well as a range of themes and issues, have emerged that typify neurodiversity advocacy (Singer 2017; Walker 2021).
≻ Most notably, neurodiversity proponents push back against the default pathologization and control of a variety of neurocognitive disabilities.
≻ They have engaged in this resistance in part by adopting social and relational models of disability, which frame disablement as the product of oppressive social environments rather than the consequence of a brain defect.
≻ As part of this resistance, furthermore, they have critiqued the very idea of the ”normal” brain or mind.
≻ In this regard, the heart of the idea of neurodiversity (and hence the neurodiversity movement) is that neurological diversity functions more like biodiversity than like pathological dysfunction: cognitive ecosystems require a diversity of minds to function.
≻ Hence, such cognitive diversity is important to support or conserve rather than eliminate or cure.
≻ The neurodiversity paradigm shifts analysis away from a focus on measurement of each person’s abilities in relation to and distance from the species norm – whereby certain people are marked as naturally defective – and moves analysis toward a focus on how normality and defect, as well as enablement and disablement, are relationally constituted.
≻ In this chapter, I situate the rise of the neurodiversity movement and what I call “neurodiversity theory” (Chapman 2019) in the broader historical context of the aforementioned discussions.
≻ My aim is, in part, to show the place and originality of neurodiversity theory in the history of critiques of psychiatric pathologization.
⚅ Day, K., & Martel, A. (2024). Neurodiversity. In C. Candido, I. Durakovic, & S. Marzban, Routledge handbook of high-performance workplaces (1st ed., pp. 148-159). Routledge. https://doi.org/10.1201/9781003328728-15
≻ All spaces – all the time – are composed of the aggregated stimuli from all senses at varying levels of intensity.
≻ For most people those levels will fall within an envelope or range that is comfortable, or at least not uncomfortable and stress inducing.
≻ However, for a percentage of the workforce those levels will be above a comfort level (hypersensitivity – an atypically high response) or below a comfort level (hyposensitivity – an atypically low response).
≻ Workplace stress for neurodiverse people is most associated with an excess of – or lack of – environmental stimuli that might emanate from sound noise, visual noise, spatial layouts, or unwanted sensory feedback through smell, touch, taste, or temperature.
≻ This chapter explores the importance of accommodating neurodiversity in the workplace and overviews the different methods that serve as guides to design for neurodiversity and the specifics of neurodivergent conditions.
⚅ Goldberg, H. (2023). Unraveling neurodiversity: Insights from neuroscientific perspectives. Encyclopedia, 3(3), 972-980. https://doi.org/10.3390/encyclopedia3030070
≻ Neurodiversity is a concept and a social movement that addresses and normalizes human neurocognitive heterogeneity to promote acceptance and inclusion of neuro-minorities (e.g., learning disabilities, attention disorders, psychiatric disorders, and more) in contemporary society.
≻ Neurodiversity is attributed to nature and nurture factors, and about a fifth of the human population is considered neurodivergent.
≻ What does neurodiversity mean neuroscientifically?
≻ This question forms the foundation of the present entry, which focuses on existing scientific evidence on neurodiversity including neurodiversity between and within individuals, and the evolutional perspective of neurodiversity.
≻ Furthermore, the neuroscientific view will be synergistically integrated with social approaches, particularly in the context of the normalization of neurodiversity and its association with the medical and social models of disability.
≻ This multidimensional analysis offers a cohesive and comprehensive understanding of neurodiversity, drawing insights from various vantage points, such as social, psychological, clinical, and neuroscientific viewpoints.
≻ This integrated approach fosters a nuanced and holistic discussion on the topic of human diversity.
≻ Brain characteristics can be an anatomical trait (e.g., structure or size of a brain region), a functional trait (e.g., the activity level of a brain system), or a combination of anatomy and function such as connectivity structure within and between brain systems.
≻ Since brain structure and function underly human perception and behavior, it is reasonable to think of the various expressions of human cognition and communication patterns as neurodiversity.
≻ While neurodiversity is often utilized to identify and label a deviation from the typical representation of neuronal and behavioral trait(s), it is important to recognize that it represents a statistical description of the population as a whole and effectively, neurodiversity exists across the entire population.


⚅ Graby, S. (2015). Neurodiversity: bridging the gap between the disabled people’s movement and the mental health system survivors’ movement? In Madness, distress and the politics of disablement (pp. 231-244). Policy Press.
≻ This chapter traces the origins and evolution of the neurodiversity movement, which consists of people with conditions (such as autistic spectrum ‘disorders,’ AD(H)D, dyspraxia, or dyslexia) which have been positioned somewhere between the traditional categories of ‘disability’ and ‘mental illness.’
≻ The neurodiversity movement has roots in, and, as will be argued, has new insights to offer to, both the disabled people’s and survivor movements.
≻ Therefore, it should be of interest to those
seeking to bridge conceptual gaps between the disabled people’s and survivor movements – such as the sticking point between them over the concept of ‘impairment’ (Plumb, 1994).
≻ Writers and activists within the neurodiversity movement are acutely aware of, and concerned with, the social construction of both ‘distress’ and ‘disability,’ and have developed their own distinct analysis of these concepts.
≻ This chapter gives an overview of some of that thinking.
≻ It draws on my own experience within the neurodiversity movement, as well as on published literature from all three movements, to illustrate the convergences and divergences between them, and finally offers some suggestions for ways forward.
⚅ Green, J. (2023). Debate: Neurodiversity, autism and healthcare. Child and Adolescent Mental Health, 28(3), 438-442. https://doi.org/10.1111/camh.12663
≻ We are at a time of unparalleled flux in our understanding of what autism is and now to respond to it, including our understanding of the role of clinical services.
≻ For any clinician working in the context of child development and child mental health services, the majority experience is probably of overwhelming demand, and then perhaps confusion.
≻ Referrals for neurodevelopmental conditions, and particularly autism, have become an increasing proportion of UK CAMHS referrals in recent years – with the consequent lengthening of wait times extending to years, sometimes equivalent to the whole length of a child’s life up until that point.
≻ Services are struggling to develop response strategies to meet user frustration, a task not helped by the fact that most interventions in current use have no good evidence of effectiveness.
≻ Consequently, a plethora of local approaches and initiatives have developed.
≻ In this article I address these clinical and related issues.
≻ I discuss current different uses of the term autism, the relation to intellectual disability, and introduce a conceptualisation of autism as emergent and transactional, which is consistent with current developmental and intervention science.
≻ This could bridge between neurodiversity and clinical perspectives and implies a framing of early intervention support that has strong clinical trials evidence and provides the basis for a rational and pre-emptive evidenced care pathway, which I describe.
⚅ Mathur, S. K., Renz, E., & Tarbox, J. (2024). Affirming neurodiversity within applied behavior analysis. Behavior Analysis in Practice, 17(2), 471-485. https://doi.org/10.1007/s40617-024-00907-3
≻ Criticisms of applied behavior analysis (ABA) from the autistic community continue to intensify and have an appreciable impact on research, practice, and conversation in stakeholder groups.
≻ ABA providers aspire to increase quality of life for autistic people; thus, it is imperative for providers to listen with humility and openness to the population we serve.
≻ Autistic individuals have unparalleled expertise in their own lives and their own communities.
≻ The concerns raised by the autistic community cannot, morally or ethically, be swept aside.
≻ There may be a misguided and harmful tendency to devalue concerns due to the speaker’s identification as autistic or due to their difference in professional credentials.
≻ The concept of neurodiversity can help the ABA field respond to these concerns and collaborate with the largest stakeholders of our services, the autistic clients we serve.
≻ This article summarizes some of the key criticisms that autistic advocates raise concerning ABA, discusses the social model of disability and the neurodiversity paradigm, and proposes practical guidance to help the field of ABA integrate neurodiversity and thereby evolve our research and practice.
≻ By openly acknowledging the criticisms against ABA and recognizing how we can do better as a field, we believe we can take practical steps towards a profession and a society that more fully embraces inclusion.
⚅ Maynard, D. W. (2024). The human spectrum: A critique of “neurodiversity.” Symbolic Interaction, symb.691. https://doi.org/10.1002/symb.691
≻ This paper represents a sociological approach to autism spectrum disorder that critiques the terms neurodiverse and it obverse, neurotypical, because they promote a cognitive approach that mystifies what is actual and real about human activity in everyday life.
≻ It is in dynamic interactional practices rather than putative cognitive states that human diversity is manifest or observable.
≻ The empirical part of the paper, following Bleuler, defines and examines “autistic talk” as a turning away from the ordinary social world or commonsense “reality,” and engaging self-oriented practices and orientations.
≻ However, the range of participants who produce such talk is not confined to those on the putative autism spectrum.
≻ Rather, that range encompasses the entire human span.
≻ If so, then a question is raised about what autism is as a “condition,” which term individualizes social difficulties rather than appreciating that they are always about diverse social actions-in-interaction.
⚅ Murray, D., Milton, D., Green, J., & Bervoets, J. (2023). The human spectrum: A phenomenological enquiry within neurodiversity. Psychopathology, 56(3), 220-230. https://doi.org/10.1159/000526213
≻ Introduction: Autism has typically been characterized by its external manifestations rather than experienced phenomenology, with consequent impacts on both research and practice.
≻ There have recently been increasing calls for more phenomenological enquiry in autism, but little actual work reported.
≻ Method: A shared participatory phenomenological self-investigation was conducted, by the four authors, of lived experience across the autistic/non-autistic divide.
≻ The sample size was chosen as necessary for the feasibility and acceptability to participants of such work in this context.
≻ Roles of “researcher” and “interviewee” were purposefully alternated between participants to establish trust and reciprocity.
≻ Initial phenomenological reduction or bracketing was applied to the description and recording of each participant’s intimate lived experience in a number of key domains across social relationships, the physical environment, development, and in adult life.
≻ These experiences were shared within dialogue to open them to investigation and questioning from the others, with alternating interviewer and respondent roles.
≻ A third step synthesized these shared observations across individuals into themes of continuity and difference.
≻ Results: A number of emergent themes, such as the need for trust and reliability, and the impact of context on regulation of emotion, sociability, and empathy, showed striking commonalities between all participants.
≻ Other themes, such as primary sensory experience and social joining, pointed up more clear differences between autism and non-autism in development and the adult world.
≻ Themes of interest-focus and attention were marked by both commonalities and difference.
≻ Conclusions: This shared phenomenological method was taken as a first step within a new area of active investigation in autistic phenomenology.
≻ It proved successful in eliciting detailed information on self-experience.
≻ The results suggested hypotheses for a new understanding of autism within the wider “human” spectrum of experience; for instance, the common basic need for trust and social connection but striking differences in sensory experience.
≻ It suggested that some characteristics long thought intrinsic to autism, such as social mis-perception and reduced empathy, may be alternatively understood as state-dependent outcomes contingent on specific contexts and interactions.
≻ Implications are suggested for testing in further research, developmental theory, and intervention practice.
⚅ Najeeb, P., & Quadt, L. (2024). Autistic well-being: A scoping review of scientific studies from a neurodiversity-affirmative perspective. Neurodiversity, 2, 27546330241233088. https://doi.org/10.1177/27546330241233088
≻Background: Historically, autism research has focused on the overrepresentation of physical and mental health problems and decreased psychological well-being in autistic people without intellectual impairment.
≻ There is a paucity of studies emphasizing what positively contributes to the well-being of autistic people.
≻ In line with a recent shift toward investigating autistic health more comprehensively, we conducted a scoping review to map emerging data on autistic well-being within a biopsychosocial context.
≻ Methods: A Lived Experience Advisory Panel coproduced the review question.
≻ The research was collated using Preferred Items for Systematic Reviews and Meta-analyses guidelines for scoping reviews (PRISMA-ScR) with predefined selection criteria.
≻ Research based on the deficit-based view of autism and not within the core principles of the neurodiversity-affirmative movement was excluded.
≻ Results: We collated 89 studies, with biological (N = 8), psychological (N = 70), and social (N = 61) factors.
≻ Alongside an increase in affirmation-focused outputs, we identified several themes: ‘Impact of Diagnosis and Self-Identity,’ ‘Self-empowering Characteristics,’ ‘Cognition,’ ‘Role of the Wider Community,’ ‘Role of Relationships and Forms of Support,’ and ‘Social Adaptations and Lessons from COVID-19.’
≻ Conclusions: While neurodiversity-affirmative perspectives on autistic well-being are increasingly recognized as an important research area, there is a need for a more stringent exploration of interlinking biopsychosocial determinants.
≻ A focused approach within future research will enhance understanding of the promotion of autistic well-being.
≻ This scoping review highlights that there is a rapidly growing field of well-being research within autistic individuals, and whilst various biological, psychological, and social factors have been identified, they also function to improve well-being through a complex meshwork of modulation.
≻ What well-being looks like for an individual is subjective, particularly within the autistic population with varying strengths and challenges.
≻ Therefore, further research is needed to decipher the different facets of wellbeing within the autism spectrum.
⚅ Pantazakos, T., & Vanaken, G.-J. (2023). Addressing the autism mental health crisis: The potential of phenomenology in neurodiversity-affirming clinical practices. Frontiers in Psychology, 14, 1225152. https://doi.org/10.3389/fpsyg.2023.1225152
≻ The neurodiversity movement has introduced a new era for autism research.
≻ Yet, the neurodiversity paradigm and the autism clinic remain largely unconnected.
≻ With the present work, we aim to contribute to filling this lacuna by putting forward phenomenology as a foundation for developing neurodiversity-affirming clinical interventions for autism.
≻ In the first part of this paper, we highlight that autistic people face a severe mental health crisis.
≻ We argue that approaches focused on reducing autistic ‘symptoms’ are unlikely to solve the problem, as autistic mental health is positively correlated with autism acceptance and perceived quality of support provided, not necessarily with lack of ‘symptomatologic severity.’
≻ Therefore, the development and dissemination of neurodiversity-affirming clinical interventions is key for addressing the autism mental health crisis.
≻ However, therapists and researchers exploring such neurodiversity-affirming practices are faced with two significant challenges.
≻ First, they lack concrete methodological principles regarding the incorporation of neurodiversity into clinical work.
≻ Second, they need to find ways to acknowledge rightful calls to respect the ‘autistic self’ within the clinic, while also challenging certain beliefs and behaviors of autistic clients in a manner that is sine qua non for therapy, irrespective of neurotype.
≻ In the second part of the paper, we introduce phenomenological psychology as a potential resource for engaging with these challenges in neurodiversity-affirming approaches to psychotherapy.
≻ In this vein, we put forward specific directions for adapting cognitive behavioral and interpersonal psychotherapy for autism.
⚃ A.8.6.2 A bibliography on neurodiversity.
⚄ These are all direct quotations. I have not put in page numbers – if you want to quote you’ll have to look up the article.
↩ Main. Top A-C D-F G-K L-O P-S T-Z
⚄ Aherne, D. (2023).
The pocket guide to neurodiversity. Jessica Kingsley Publishers.
≻ My name is Daniel Aherne, and this is my guide to the fascinating and hotly debated topic of neurodiversity.
≻ In my professional and personal experience, one of the biggest things we can do to improve someone’s environment is to provide education and awareness to those around them.
≻ Greater empathy for and awareness of other people’s differences can radically improve their day-to-day experiences.
≻ This philosophy is what motivates me to educate people about neurodiversity.
≻ And it’s why I’ve written this guide.
≻ Common neurodivergent identities include autism, dyslexia, dyspraxia (DCD), ADHD, Tourette’s syndrome, dysgraphia and dyscalculia.
≻ There are lots of diagnostic overlaps between different neurotypes, and it is becoming increasingly common for people to identify with two or more of the neurotypes.
≻ In this guide, I will focus on explaining more about autism, dyslexia, dyspraxia and ADHD; by understanding these four neurotypes a little better, you will be well on your way to becoming more neuro-inclusive.

⚄ Armstrong, T. (2011).
The power of neurodiversity: Unleashing the advantages of your
differently wired brain.
(published in hardcover as
Neurodiversity). Da Capo Lifelong Books.
≻ The book begins with a chapter that summarizes eight basic principles about neurodiversity, including the idea of “niche construction,” which, like a beaver building a dam, provides opportunities for neurodiverse individuals to create suitable lifestyles for themselves that seek not so much to fit into the world around them as to make the world accommodate itself to their needs, styles, and assets.
≻ The next seven chapters take each of the brain conditions listed above in turn and focus on the strengths that I’ve observed in the literature.
≻ Especially interesting to me is the way in which these conditions are regarded in other cultures, or might have proved useful in times past (including prehistoric times).
≻ This serves to highlight another of my central principles from chapter 1: whether you are regarded as disabled or gifted depends largely on when and where you were born.
≻ I am convinced that not enough attention has been given to the cultural relativity of disability labels and that there are good reasons why these conditions are still in the gene pool.
≻ In each of the seven chapters, I also examine how to construct niches using assistive technologies (e.g., spell checkers and text-to-speech software for dyslexics), good career choices (e.g., the computer field for people with autism), human resources (e.g., a life coach for people with ADHD), and specific strategies (e.g., mindfulness meditation for people with anxiety disorders).
≻ In chapter 9, I look at neurodiversity applied to children and education, noting that special education programs up until now have been isolating, stigmatizing experiences for many kids and that a new type of inclusive neurodiverse classroom, consisting of kids with and without labels, is a more suitable learning environment for all children.
≻ Finally, in chapter 10, I write about the future of neurodiversity, examining a business, for example, that hires people with Asperger's syndrome to test computer software because they do a better job than so-called neurotypicals.
≻ I also look at the increasing threat that genetic engineering and prenatal screening pose in potentially eliminating neurodiverse people from the planet.
≻ An appendix provides a list of helpful books, videos, organizations, and assistive technologies for each of the seven brain differences covered in this book.
⚄ Arnold, L. (2017). A brief history of 'neurodiversity' as a concept and perhaps a movement.
Autonomy, the Critical Journal of Interdisciplinary Autism Studies, 1
(5).
≻ The term Neurotypicality was concocted, first as a satire in the form of a thought experiment, of what it would be like if mainstream thinkers (for want of a better word) were categorised as mentally ill, a bit like Samuel Butler’s satire Erewhon (Butler, 1872).
≻ There the notion was to try and give the non-autistic individual a sense of what it was like to be pathologised and stigmatised, in a similar way to Finkelsteins famous parody of the village. (Finkelstein, 1975)
≻ Alas ‘neurotypical’ as a faux binary opposite to ‘neurodiversity’ has since become reified into a term used equally amongst an autistic community and the self-same academic psychiatric community it parodied.
≻ The word has become colonised by the enemy and as a consequence I prefer simply to refer to non-autistic people as not being autistic does not necessarily imply that everybody else is within that bell curve of ‘neurotypicality.’
⚄ Astle, D. E., Holmes, J., Kievit, R., & Gathercole, S. E. (2022). Annual research review: The transdiagnostic revolution in neurodevelopmental disorders.
Journal of Child Psychology and Psychiatry, 63 (4), 397–417.
https://doi.org/10.1111/jcpp.13481
≻ Transdiagnostic studies focus on characteristics and mechanisms that may not align with any conventional diagnostic category.
≻ Many different study designs have yielded transdiagnostic insights into NDDs.
≻ Figure 1 represents these designs as a spectrum ranging from studies that focus exclusively on standard diagnostically defined disorders through to data-driven discovery studies with no a priori clinical or subclinical selection criteria.


⚅⚀ In this article, we argue that diagnostic taxonomies that classify individuals in terms of discrete categories are ill-suited to do this.
≻ Evidence-based transdiagnostic approaches provide compelling alternatives with the flexibility to capture the true heterogeneity of NDDs in the population at large.
⚄ Baron-Cohen, S. (2017). Editorial perspective: Neurodiversity – a revolutionary concept for autism and psychiatry.
Journal of Child Psychology and Psychiatry, 58 (6), 744–Basic747.
https://doi.org/10.1111/jcpp.12703
≻ This editorial focuses on the question of whether autism is properly characterised as a disorder and whether the neurodiversity framework should be embraced.
≻ Many in the autism community adopt the neurodiversity framework, coining the term ‘neurotypical’ to describe the majority brain.
≻ Steve Silberman’s terrific book
Neurotribes is a kind of manifesto for the neurodiversity movement, encouraging us to recognise autism as an example of diversity in the set of all possible brains, none of which is ‘normal’ and all of which are simply different.
≻ Left-handers are an example of neurodiversity in a majority right-handed world, and left-handers used to be seen as a pathological condition that needed correction.
≻ In the same way, the concept of neurodiversity challenges whether people with autism should automatically be ‘treated’ and ‘normalised.’
≻ ‘Disorder’ should be used when there is nothing positive about the condition, or when despite trying different environmental modifications, the person is still unable to function.
≻ ‘Disease’ should be used when the biomedical mechanistic cause of a disorder becomes known, perhaps through medical testing or through scientific research.
≻ ‘Disability’ should be used when the person falls below an average level of functioning in one or more psychological or physical functions, and where the individual needs support or intervention.
≻ ‘Difference’ should be used when the person is simply atypical, for biological reasons, relative to a population norm, but where this difference does not necessarily affect functioning or well-being.
≻ It will be important to see how the concept of neurodiversity is applied to the 300 diagnoses currently all called ‘disorders’ in DSM-5, and if it revolutionises both the science and the practice of psychiatry.
⚄ Bertilsdotter-Rosqvist, H., Chown, N., & Stenning, A. (Eds.). (2020).
Neurodiversity studies: A new critical paradigm. Routledge.
≻ Scholars have now ‘amassed overwhelming evidence of the extent to which the myths of the ideal rational person and the ‘universality’ of propositions about human nature have been oppressive to those who are not European, white, male, middle class, Christian, able-bodied, thin, and heterosexual’ (Ellsworth, 1989, p. 304).
≻ The concept of neurodiversity usually refers to perceived variations seen in cognitive, affectual, and sensory functioning differing from the majority of the general population or ‘predominant neurotype,’ more usually known as the ‘neurotypical’ population.
≻ The ontological assumption of neurodiversity is often contrasted with the ideological position that there is a recurrent ‘normal’ cognitive, affective, and sensory type, otherwise known as the normal human being or the ‘normate’ (Garland Thomson, 1997), as defined in the first half of the twentieth century, by way of the prerogative of psychologists who were living in the shadow of eugenics.
≻ The attribute of neurodivergence may also be applied – more problematically – to individual people.
≻ As Nick Walker says, ‘Diversity is a trait possessed by a group, not an individual’ (2014) and to talk of individuals as neurodiverse is to situate them as ‘other’ to the norm (as well as being, in our opinion, nonsensical).
≻ Those who share a form of neurodivergence – such as bipolar or hearing voices – may be referred to as a ‘neurominority.’
≻ We use the expressions ‘neurodivergence’ and ‘neurodivergent conditions’ simultaneously and as alternatives to the idea of ‘persons with disorders’ (conceived as an inherently harmful condition that impacts on a person’s flourishing) that is encompassed by standard medical models of conditions such as autism and dyslexia.
≻ This is similar to the way in which autism self-advocates have, since the 1990s, argued for identity-first language in the discussion of autism.
≻ In this way, we are concerned with providing a new theorisation of conditions that are understood as impacting on the individual’s sense of identity, alongside differences from standard forms of perceiving and responding to the world.
≻ This book aims to problematise neurotypical domination of the institutions and practices of academic knowledge production, by questioning the boundaries between the predominant neurotypes and their ‘others.’
≻ We address the cultural and social processes of ‘cognitive othering’ through which they have arisen in the West during the past 100 years.
≻ The creation of boundaries – both by the neurotypical and the neurodivergent – is always subject to cultural and ideological pressures.
≻ By using neurodivergence as a position with epistemological and ethical implications we will decentre – if temporarily – dominant perspectives.
⚄ Blume, H (1998 September 30). On the neurological underpinnings of geekdom.
The Atlantic Monthly.
≻ With so much going on in a brain, the argument goes, the occasional bug is inevitable: hence autism and other departures from the neurological norm.
≻ ISNT [the now defunct Institute for the Study of the Neurologically Typical] suggests another way of looking at this.
≻ Neurodiversity may be every bit as crucial for the human race as biodiversity is for life in general.
≻ Who can say what form of wiring will prove best at any given moment?
⚄ Botha, M., & Gillespie-Lynch, K. (2022). Come as you are: Examining autistic identity development and the neurodiversity movement through an intersectional lens.
Human Development, 66 (2), 93–112.
https://doi.org/10.1159/000524123
≻ Singer intended for neurodiversity to be a new category of intersectionality.
≻ However, intersectionality has been neglected in autism research and practice.
≻ This paper aims to inform an intersectional approach to autism by exploring autistic identity development in relation to other marginalized identities.
≻ As we learn more about the twisted origins of the diagnostic category “autism,” it becomes increasingly unsurprising that many autistic people have called for a fundamental shift in how autism research and practice are conducted.
≻ A central premise of our paper is that autistic people have reframed the diagnostic category “autism,” once conceptualized as an innate inability to connect socially, into a social identity which they use as a rallying call for collective action, often under the banner of the neurodiversity movement (Kapp, 2020).
≻ Singer intended for neurodiversity to be used as a new category of intersectionality, a term coined by Crenshaw (1989) to show that people with more than one marginalized identity (e.g., Black women) experience and lack legal protection from compounded forms of discrimination.
≻ By providing a framework to critique discrimination based on “neurological differences,” the term neurodiversity called forth a new rights-based movement, the neurodiversity movement.
≻ The neurodiversity movement challenges the notion that autistic people experience innate social impairments, highlighting the relational nature of social difficulties and reframing autism as a valuable minority identity that needs no cure (Kapp et al., 2013; Kapp, 2020).
≻ Unlike the social model of disability, which attributes disability-related challenges solely to oppressive societal attitudes and structures, the neurodiversity movement frames neurological diversity as invaluable for societal progress and yet inherently challenging at times, meaning that autism can both be an identity, and an embodied disability with aspects of impairment (Bailin, 2019; Baker, 2011; Ballou, 2018).
≻ It is vital to ensure that the neurodiversity movement does not become another analytical tool for disability and identity that is wrapped up in and reproduces white supremacy, cis-heteronormativity, classism, cisgenderism, or sexism.
≻ Emancipation from any system of oppression means working to undo all systems of oppression, because although they are in some ways distinct, they are inseparable, and work to maintain each other (Lorde, 2003).
≻ At its core, neurodiversity is about the deserving dignity which should be afforded to all people despite neuronormative ideas of functioning and traditional constructions of independence and productivity.
≻ The lack of a clear or singular biological basis for autism has led an increasing number of researchers to assert that the diagnostic category autism is, at least partially, socially constructed (Chapman, 2020; Grinker, 2015; Lord et al., 2020); that is, autistic people are grouped together by very real characteristics which have been assigned meanings that change across time and cultures.
≻ Thus, even if the focus on genetic etiology provides a specific set of genes that are predictive of autism (which it has not yet), one still could not understand autism without understanding how it is socially constructed.
≻ This emerging recognition that autism is, at least partially, socially constructed moves our understanding of autism closer to intersectionality theory.
≻ Through claims of biological determinism of intelligence, morality, and other characteristics, scientific racism has a long history of twisting data to categorize people who are not white as “separate” and “inferior” races (Gould & Gold, 1996) – a tradition which is rooted in eugenics and academically sanctioned (Teo, 2011).
≻ The idea that there is such a thing as a “normal” person or a “normal” path through development is also a socially defined construct (Fenton & Krahn, 2007).
≻ The idea of “normal,” modern statistics, and eugenics share a common root. a eugenic tradition which persisted with Herrnstein and Murray’s 1994 text
The Bell Curve: Intelligence and Class Structure in American Life. Its authors used a statistical distribution to determine who was “worthy” of full consideration within American society, and while not advocating for forced sterilization, argued for mandates and policy which indirectly controlled populations.
≻ Intersectionality teaches us that we must understand differences within the autistic community if we wish to help all autistic people experience the dignity they deserve.
≻ Dekker (2020), who founded InLv, where the idea of neurodiversity emerged, wrote that the neurodiversity movement was never intended to exclude or shame autistic people who view autism negatively and/or wish they are not autistic.
≻ As Chapman (2021) suggested, the neurodiversity movement should embrace autistic diversity while seeking empirical support for its central premise that diversity improves functioning (e.g., stronger evidence that more diverse groups are more creative but also experience more conflict; Torchia et al., 2015).
≻ To understand autistic identity development, including potential impacts of the neurodiversity movement, we must study individual and group successes and struggles in relation to shifting social contexts.
≻ Research should examine socialization and cultural factors that could explain unexpected relationships between minority stress and outcomes, ideally with longitudinal mixed-methods design.
≻ Such work should assess structural and everyday stigma, family socialization practices and autistic cultural traditions in relation to mental health outcomes, but also positive characteristics we know to be important for development, like authenticity, pride, belonging, and collective advocacy.
⚄ Brown, H. M., Stahmer, A. C., Dwyer, P., & Rivera, S. (2021). Changing the story: How diagnosticians can support a neurodiversity perspective from the start.
Autism, 25 (5), 1171–1174.
https://doi.org/10.1177/13623613211001012
≻ The diagnostic entity of autism is a subjective construct used by society to interpret and categorize behaviour, affect and ways of thinking – a sort of story or narrative (Duffy & Dorner, 2011).
≻ The way we share this diagnostic story with families will guide their thinking about ‘how to accommodate and respect autistic children – and how to love them.
≻ Or they help autistic[s] understand themselves, [and learn] how to get on in a world of neurotypicals’ (Hacking, 2009, p. 502).
≻ Dominant autism narratives, including those shared by the diagnostician at the initial diagnosis, will be heard and internalized by families, autistic children and society as a whole.
≻ The medical model has created stories of autism in which ‘autistic people are inherently inferior to nonautistic people, [that autistics] lack something fundamental to being human, and that autism is something to be fixed, cured, controlled or avoided’ (BottemaBeutel et al., 2020, p. 8).
≻ Solely deficit-framed descriptions often miss the strengths that can be associated with autism.
≻ While autistic children often have more challenges than neurotypical children, the overall well-being of autistic children and their families is harmed when we frame autism in terms of deficits alone.
≻ The diagnostician can help parents reframe negative messaging while reassuring parents that they will learn how to harness the strengths of both their child and themselves to promote the well-being of their family.
⚄ Burge, M. (2012).
The ADD myth: How to cultivate the unique gifts of intense
personalities.
Conari Press.
≻ Ms. Burge offers a strategy she hopes may help cure the “epidemic” of ADD.
≻ She warns us to stop medicalizing what is often basically normal behavior and to stop over-treating with unnecessary and potentially harmful medication.
≻ She offers an alternative approach for dealing with the “myth” of ADD that accepts and accommodates the human variability it represents, rather than pathologizing and treating as illness all hyperactivity, impulsivity, and distractability.
≻ Burge decries the ADD “myth” as a medicalization of emotional intensity.
≻ She would prefer we accommodate human difference, rather than explain it away as an ill to be casually treated with a pill.
≻ Burge normalizes what the DSM pathologizes.
≻ She recommends that we not be preoccupied with the limitations and impairments that come with ADD.
≻ Instead, Burge focuses on the benefits inherent in an ADD lifestyle, and suggests ways to enhance them further and to limit and cope with the concomitant difficulties.
⚄ Chapman, R. (2021, August 18). Negotiating the neurodiversity concept: Towards epistemic justice in conceptualising health.
Psychology Today. Retrieved March 18, 2023, from
https://www.psychologytoday.com/ca/blog/neurodiverse-age/202108/negotiating-the-neurodiversity-concept
≻ As Meadows puts it, on their understanding, “The neurodiversity paradigm says: there is no such thing as a normal brain.
≻ Variation in neurology is natural, and none is more right or wrong than another.”
≻ Meadows' aim here is to be inclusive in who “counts” as neurodivergent, and I think that aim is noble.
≻ But I understand the requirements of inclusivity differently.
≻ For me, rejecting the idea of a single kind of “right” brain or mind (which I agree with) does not imply that there can be no “wrong” kinds.
≻ By analogy: multiculturalism rejects the idea that there is any “right” culture, but it's still consistent for multiculturalists to think totalitarian culture is “wrong.”
≻ Similarly, Kassiane Asasumasu, who coined the term “neurodivergent,” emphasised that “Neurodivergent refers to neurologically divergent from typical,” which includes “Autistic people. ADHD people. People with learning disabilities. Epileptic people. People with mental illnesses. People with MS or Parkinsons or apraxia or cerebral palsy or dyspraxia or no specific diagnosis but wonky lateralization or something.”
≻ As she goes on, then: “It is not another damn tool of exclusion.
≻ It is specifically a tool of inclusion.”
≻ Yet while Meadows seems to take this to mean being inclusive in wholly depathologising all kinds of currently pathologised minds, Asasumasu sees mental or neurological illness as an aspect of (some kinds of) neurodivergence.
≻ For Asasumasu – and while I suspect she would sympathise with Meadows' timely critique of the co-option of neurodiversity paradigm vocabularies – including illness within the paradigm is part of inclusion, not its antithesis.
⚄ Clouder, L., Karakus, M., Cinotti, A., Ferreyra, M. V., fierros, G. A., & Rojo, P. (2020). Neurodiversity in higher education: A narrative synthesis.
Higher Education, 80 (4), 757–778.
https://doi.org/10.1007/s10734-020-00513-6
≻ This narrative synthesis focuses specifically on intellectual impairment but adopts an alternative, nuanced term of ‘neurodiversity,’ an umbrella term, originally coined in relation to autism, for several conditions traditionally pathologized and associated with a deficit, including dyspraxia, dyslexia, attention deficit hyperactivity disorder, dyscalculia, autistic spectrum and Tourette syndrome (Singer 1999).
⚄ Costandi, M. (2019, September 12). Why the neurodiversity movement has become harmful. Aeon Essays. Aeon Magazine. Link.
↩ Main. Top A-C D-F G-K L-O P-S T-Z
⚄ Dawson, G., Franz, L., & Brandsen, S. (2022). At a crossroads – Reconsidering the goals of autism early behavioral intervention from a neurodiversity perspective. JAMA Pediatrics, 176(9), 839.
https://doi.org/10.1001/jamapediatrics.2022.2299
≻ The neurodiversity movement is akin to a civil rights movement.
≻ Among its goals are reducing stigma, increasing accessibility, and ensuring that autistic individuals' voices are represented in decisions about autism research, policy, and clinical practice.
≻ The neurodiversity movement is having a growing influence on the scientific community, as evidenced in the recent pause in a large autism genetic study based on concerns raised by the autism community.
≻ It is also affecting autism practitioners as, increasingly, parents are expressing reservations about enrolling their child in early intervention programs, citing concerns that such programs do not value neurodiversity and, instead, prioritize changing their child's behavior to fit neurotypical norms.
≻ Neuroscience has underscored the plasticity of the brain in early development and suggests that expanding the repertoire of skills of an autistic child to include social reciprocity, language and communication, self-regulation, and adaptive skills through early intervention is fully compatible with encouraging autistic strengths and teaching self-advocacy skills.
≻ In the future, the use of a strengths-based approach to define outcome measures that emphasizes the unique abilities of each autistic individual will promote positive self-esteem and potentially help reduce the high rates of depression and anxiety experienced by autistic individuals.
≻ The neurodiversity perspective urges the field of autism intervention research to reframe the goal of early intervention as the promotion of a diversity of adaptive skills and traits that will lead to a fulfilling life as an autistic individual.
⚄ Dekker, M. (2020). From exclusion to acceptance: Independent living on the autistic spectrum. In S. K. Kapp (Ed.),
Autistic community and the neurodiversity movement (pp. 41–49). Springer Singapore.
https://doi.org/10.1007/978-981-13-8437-0_3
≻ It is important to note that InLv’s notion of neurodiversity was different from the “neurodiversity paradigm” that many contemporary activists subscribe to.
≻ These days it is often held that there is no such thing as a brain that is “less” or “broken” because “all neurologies are valid.”
≻ By contrast, neurodiversity as an aspect of biodiversity includes and accepts people with suboptimal neurological configurations.
≻ While autistic people who would have preferred to be “cured” if possible were a minority in the InLv community, we never excluded or denounced them.
≻ As one of the Autscape organization's directors, it makes me happy to see InLv's spirit of inclusion and acceptance continue there.
⚄ Doyle, N. (2020). Neurodiversity at work: A biopsychosocial model and the impact on working adults.
British Medical Bulletin, 135 (1), 108–125.
https://doi.org/10.1093/bmb/ldaa021
≻ The term ‘Neurodiversity’ was originally developed by stakeholders influenced by the social model of disability.
≻ It was based on ‘Biodiversity,’ a term primarily devised for political ends: to advocate for conservation of all species, since a high level of biodiversity is considered desirable and necessary for a thriving ecosystem.
≻ Neurodiversity advocates adapted this principle to argue that society would benefit from recognizing and developing the strengths of autism or dyslexia (for example) instead of pathologizing their weaknesses.
≻ A definition has emerged for psychologists and educators which positions neurodiversity ‘within-individuals’ as opposed to ‘between-individuals.’
≻ To elucidate: the psychological definition refers to the diversity within an individual’s cognitive ability, wherein there are large, statistically-significant disparities between peaks and troughs of the profile (known as a ‘spiky profile,’ see fig. 1).
≻ A ‘neurotypical’ is thus someone whose cognitive scores fall within one or two standard deviations of each other, forming a relatively ‘flat’ profile, be those scores average, above or below.
≻ Neurotypical is numerically distinct from those whose abilities and skills cross two or more standard deviations within the normal distribution.

⚅⚀ To refer to individuals, the terms ‘neurodivergent’ ‘neurodifferent’ and ‘neurodiverse’ are in current use both academically and for self-identification; this is a matter of stakeholder debate.
≻ In recognition of the lack of consensus regarding which term is more appropriate, all may be referred to interchangeably, asking individuals how they prefer to identify.
≻ The Neurodiversity movement holds ambitions of equal rights for members, appreciation of the diversity of human cognition and political power to break down structures of exclusion.
≻ Nowhere has this argument been more compelling to date than the innovative technology, finance and defence industries, where programs to deliberately hire neurominority employees are becoming more frequent as talent strategies, rather than social responsibility projects.
≻ The disparity between the language and assumptions of psychological and medical ‘experts’ and the lived experience of ‘stakeholders’ has led to dissent and conflict both between and within these groups.
≻ Within the biopsychosocial model of neurodiversity, understanding work-related intervention and treatment becomes more about adjusting the fit between the person and their environment than about treating a disorder.
≻ Critical review of the extant biopsychosocial research supports the social model proposition that the individual is not disabled, but the environment is disabling.
≻ This article has provided an overview of the neurodiversity employment picture; namely high percentages of exclusion juxtaposed against a narrative of talent and hope.
≻ Understanding the importance of nomenclature, sensory sensitivity and the lasting psychological effects of intersectional social exclusion is key for physicians wanting to interact confidently and positively with neurominorities.
≻ The proposed biopsychosocial model allows us to provide therapeutic intervention (medical model) and recommend structural accommodation (legislative obligation) without pathologization (social model).
≻ In other words, we can deal pragmatically with the individuals who approach us and strive for the best outcomes, given their profile and environment.
⚄ Doyle, N. (2022, August 26). Hidden figures in neurodiversity: Judy Singer?
Forbes.
https://www.forbes.com/sites/drnancydoyle/2022/08/26/hidden-figures-in-neurodiversity-judy-singer/?sh=492c30316544
≻ Judy Singer completed her seminal thesis in 1998, the first academic sociological inquiry into the growing Autistic Self-Advocacy Movement.
≻ Her work was based on participant observation of online autistic self-advocacy groups and was subtitled “a personal exploration of a new social movement based on neurological diversity.”
≻ Singer initially proposed “Neurodiversity” as banner term to name to the movement that was emerging not just from the Autistic sphere, but also attracting other neurominority groups, e.g. those labelled with ADHD and the “Dys”es.
≻ All of these groups were developing the self-confidence to challenge the prevailing Bible of Psychiatry, the DSM’s bleak litany of deficiencies unbalanced by their strength, and clearly needed an umbrella term for their common cause.
≻ The Neurodiversity Movement has become a powerful minority-rights campaign, inspiring the world’s largest companies to radically shift their hiring and talent management practices.
≻ A thriving cottage industry has developed to advise employers through consultancy and professional services.
≻ The neurodiversity paradigm is redesigning scientific enquiry: instead of just scanning the brains of neurodivergent kids to find the bits that are broken, we are questioning homogeneity of thought.
≻ We are exploring the potential of what Dr Helen Taylor has since developed and termed “complementary cognition.”
≻ These changes are influencing disciplines from psychology and psychiatry through to archaeology and anthropology, and moving the focus from “what is wrong with this individual” to “what social barriers are turning difference into disability and exclusion.”
≻ I stumbled on disability studies when I was studying sociology, and I cried all night at the first book I read, when I realised we had a disability in the family, even though I didn’t know what it was.
≻ At that time I hadn’t even heard of Asperger’s Syndrome or an Autistic Spectrum.
≻ When I finally had my Aha! Moment, I was beside myself with excitement, and using all the resources of my university did a massive literature search to find the experts, and found absolutely nothing!
≻ Which is when it struck me. “OMG!
≻ The expert might have to be me!.” So I signed up for Honours to write a thesis.
≻ I was limited to just 15,000 words, so it concentrated my mind wonderfully.
≻ I was absolutely confident that this new movement was destined to be last great “liberation” movement of the 20th century in the mold of the women’s and gay movements.
≻ So I gave it my all!
≻ I wanted the world to understand.
≻ Not that I had any expectation that anyone was even going to read my work.
≻ Australia’s post-colonized “Cultural Cringe” means we don’t recognize our own, unless they are recognized in the Northern Hemisphere first.
≻ Meanwhile, the North extracts value from the South in whatever form it can.
≻ I was considered “eccentric”, my work was ignored, and I moved on to my other burning issues, including Australia’s shocking abuse of unemployed people, older women, homeless people, and tenants.
≻ While I am flattered by the attention I have latterly received for this word, I would like to be recognized for my true achievement, a roadmap for the movement that is actually redefining how we see ourselves as humans.”
⚄ Doyle, N., Hough, L., Thorne, K., & Banfield, T. (2022). Neurodiversity. In G. C. Liell, L. F. Jones, & M. J. fisher,
Challenging bias in forensic psychological assessment and testing (1st ed., pp. 329–357). Routledge.
https://doi.org/10.4324/9781003230977-22
≻ There is no internationally agreed definition of neurodivergence, however, a recent UK Criminal Justice Joint Inspectorate Neurodiversity Review (CJJI, 2021) considered it an umbrella term referring to the group of conditions falling under the category of neurodevelopmental disorders (NDDs).
≻ These incorporate learning difficulties and disabilities (LDDs) generally including: Learning Disability, Dyslexia, Dyscalculia, and Dyspraxia (also known as developmental coordination disorder, DCD); clinical conditions, such as Attention Deficit Hyperactivity Disorder (ADHD, including ADD), Autism Spectrum Conditions (ASC), Developmental Language Disorder (DLD, including Speech and Language Difficulties), Tic Disorders (including Tourette’s Syndrome and Chronic Tic Disorder) and cognitive impairments due to acquired brain injury (ABI).
≻ Some definitions of neurodivergence incorporate disorders affecting executive functioning and cognition, whilst others reference Deafness and Sight Loss.
≻ The implication of the Neurodiversity model therefore is that there are essentially two types of people: “neurotypical”, whose cognitive abilities and neurological functions fit within one or two standard deviations of the statistical “norm”; and a sizeable neurominority, estimated at 15–20%, whose profiles are neurodivergent from the norm, itself defined by the prevailing socio-historical context.
≻ The Neurodiversity movement thus aligns itself with diversity and inclusion, seeking similar equity to race, gender, and LGBTQIA2S1 + movements, and has a relationship with other disability inclusion approaches; for example, the Deaf Community and corresponding Deaf Culture literature
⚄ Dwyer, P. (2022). The neurodiversity approach(es): What are they and what do they mean for researchers?
Human Development, 66 (2), 73–92.
https://doi.org/10.1159/000523723
≻ The neurodiversity approaches are an alternative to the medical model.
≻ Judy Singer (2016), who coined the term “neurodiversity,” suggested appropriating and modifying the metaphor of biodiversity:Why not propose that just as biodiversity is essential to ecosystem stability, so neurodiversity may be essential for cultural stability?
≻ Why not strategically argue that the nurturing of neurodiversity gives society a repository of types who may come into their own under unforeseeable circumstances (location nos. 1079–1081).
≻ These neurodiversity approaches are not solely about autism; they can be applied to a wide range of different sorts of disabled minds and brains.
≻ Unfortunately, defining “neurodiversity” is not particularly easy.
≻ Walker (2014) distinguishes between three different meanings of the term. first and most straight-forwardly, “neurodiversity” can simply refer to the reality that diverse minds and brains exist, just as “biodiversity” refers to the factual reality of biological diversity.
≻ In this factual sense, even groups of neurotypical people are neurodiverse, as no two individuals have exactly the same mind or brain.
≻ The other usages of “neurodiversity” are much harder to define.
≻ Walker (2014) identifies a specific theoretical perspective she refers to as the “neurodiversity paradigm,” though others (e.g., Kapp, 2020; Russell, 2020) prefer the term “neurodiversity framework.”
≻ This article will use the terms “neurodiversity approach” and “neurodiversity approaches.”
≻ Walker distinguishes the neurodiversity approaches from the “neurodiversity movement,” an activist movement that seeks to advance the rights and welfare of neurologically atypical disabled people, or “neurodivergent” people.
≻ Instead of there being one singular neurodiversity paradigm, it might be more accurate to speak of multiple “neurodiversity approaches.” some opponents of the neurodiversity approaches claim they take even more radical stances.
≻ Arguments against the neurodiversity approaches often claim the approaches oppose access to supports or that they do not consider autism to be a disability, which are not positions taken by most neurodiversity advocates (den Houting, 2019).
≻ It seems reasonable to propose that a neurodiversity approach operating in a middle ground between the extremes of the strong social and medical models would likely be both more practically useful and less controversial than a more radical, strong social model-aligned approach.

⚅⚀ In this interactionist neurodiversity framework, intervention could operate at the individual level (e.g., stimulant medications for ADHD individuals), by changing the environment (e.g., removing environmental distractors), or by changing both the environment and the individual.
≻ The decision between these alternatives should not be based on whether the individual or environment is perceived to be the ultimate cause of the disability but based on which intervention would best enhance quality of life.
≻ Neurodivergent individuals will likely have crucial insights regarding which approach would be most helpful for them, and their preferences should be respected to the extent that the person can communicate them.
≻ Although the neurodiversity approach proposed here would allow interventions to attempt to promote wellbeing by teaching adaptive skills to neurodivergent individuals, it would not endorse interventions that aim to “normalize” neurodivergent people by simply making them more like neurotypicals.
≻ An optimal neurodiversity approach should probably be understood to require acceptance of the disabled individual and use of respectful language to describe them.
≻ Even if the disabled individual is to have access to interventions that might aim to teach them new skills, the disabled individual should not feel they are deficient, but that they are accepted and valued as they are.
≻ Areas of challenge can and should of course be acknowledged along with strengths, but there is a considerable difference between acknowledging that someone experiences challenges and dismissing them as “disordered” due to their “deficits.” it does not seem reasonable to apply the neurodiversity approaches to all neurodivergent people.
≻ For example, someone with a cancerous brain tumor could be considered neurodivergent, but it would seem absurd to treat their tumor using any approach other than the medical model.
≻ Chapman (2020b) later introduces the concept of “neurotype dysphoria” to describe people who do not identify with and who desire to change their neurotype.
≻ In addition to neurodivergent individuals who desire to be neurotypical, “neurotype dysphoria” would also include neurotypicals who desire to be more neurodivergent, which thus puts neurotypical and neurodivergent people on a theoretically even footing.
≻ While interventions capable of effectively transforming someone’s neurotype might not be available to most people today, under a “neurotype dysphoria” informed approach, it might someday become possible for people to choose to pursue a sort of neurotype transition, similarly to how individuals experiencing gender dysphoria might pursue a gender transition.
≻ Neurodiversity approaches must also recognize that some neurotypes do have a less socially constructed, more genuinely discrete existence based on genetic variants.
≻ Though even these genetic classifications can be heterogeneous not only phenotypically (e.g., Hamner et al., 2019; see also Castelbaum et al., 2019) but also genetically (e.g., due to mosaicism, repeat length), categories such as Down syndrome and fragile X syndrome are clearly more biologically discrete than autism.
≻ However, whether diversity is dimensional or discrete, it is still diversity, and thus fundamentally seems compatible with a neurodiversity approach.
≻ One obvious practical ramification of neurodiversity approaches is that the scope of research inquiry should be expanded to include the environment around the disabled person.
≻ This article has offered researchers an overview of the neurodiversity approaches, as well as discussion of ongoing theoretical controversies regarding the approaches.
≻ Although the neurodiversity approaches are evolving and although their relation to the social model of disability remains a subject of debate, it is here proposed that the optimal neurodiversity approach should take a middle ground between the social and medical models, as suggested by Singer (2016).
≻ This neurodiversity approach would consider disability as emerging from an interaction of individual and context, and it would allow interventions to either change individuals in limited ways (e.g., teaching skills, using medication to manage difficulties) or to change environments and societies (see Table 1).
≻ This neurodiversity approach would not permit interventions aiming to normalize or cure disabled individuals.
⚄ Evans, B. (2017).
The metamorphosis of autism: A history of child development in Britain.
≻ Autism is an essential concept used in the description of child development and its variances.
≻ Yet the phenomenal success of autism diagnoses is relatively recent.
≻ Today, autistic spectrum disorder is regarded as a developmental condition with genetic and biochemical correlates that often persists into adulthood.
≻ The condition of autism was thought to affect just 4 per 10,000 people and was thus considered extremely rare.
≻ There were some psychological specialists who wrote on the subject of autism in the 1960s, but they largely regarded ‘autism’ as a normal developmental stage in the formation of human relationships, characterised by hallucinatory and imaginary thinking, which they thought some children were never able to overcome.
≻ This is not the ‘autism,’ or autistic spectrum, that we know today.
≻ In fact, an important part of this book covers the major transition, indeed complete reversal, in the meaning of autism that occurred in the late 1960s and 1970s, and was fully embraced by the 1990s.
≻ In this book, I argue that it was this reversal in the meaning of autism that enabled the expansion of the category; the growth in diagnoses; the expansion of health, educational and social services for individuals diagnosed with autism; and the general cultural phenomenon that autism has become today.
≻ In early 2015, a team of researchers from Canada, USA, China and Sweden concluded that ‘substantial genetic and clinical heterogeneity exists in ASD and that much larger surveys will need to be completed to completely understand the genetic architecture of ASD.’
≻ It would be hard to find a clearer advertisement for the idea of neurodiversity.
⚄ Farquhar-Leicester, A. L., Tebbe, E., & Scheel, M. (2022). The intersection of transgender and gender-diverse identity and neurodiversity among college students: An exploration of minority stress.
Psychology of Sexual Orientation and Gender Diversity.
https://doi.org/10.1037/sgd0000603
≻ Overall, findings from this study underscore the need for continued research into the experiences, mental health, and academic outcomes for TGD undergraduate students who are ND.
≻ It is notable that our use of a person-centered approach led to the identification of important within-group differences related to gender- and neurodiversity-based minority stress experiences.
≻ Furthermore, membership in the emergent profiles was linked to other aspects of social identity, with clear clusters along dimensions of race and ethnicity, gender, and socioeconomic status within the profiles.
≻ As a result, we echo the numerous calls for future research and scholarship (e.g., Cole, 2009; Moradi & Grzanka, 2017) to continue to attend to the ways in which multiple, intersecting systems of oppression and privilege shape health disparities and issues of equity in higher education.
⚄ Fletcher-Watson, S. (2022). Transdiagnostic research and the neurodiversity paradigm: Commentary on the transdiagnostic revolution in neurodevelopmental disorders by Astle et al.
Journal of Child Psychology and Psychiatry, 63 (4), 418–420.
https://doi.org/10.1111/jcpp.13589
≻ In its simplest form, neurodiversity is the fact that humans vary in their neurological make-up and that this variability dictates the ways in which we process information – and therefore our experiences of and responses to the world.
≻ These differences can be thought of in terms of dimensional variability between individuals, but also as drivers of clusters, or ‘neurotypes’ – mapping on to the dimensions and clusters of transdiagnostic research.
≻ Individuals thought to be part of the most common neurotype are often described as ‘neurotypical,’ while other groups – overlapping with diagnostic categories such as ADHD, autism, Tourette syndrome and so on may be referred to as neuro-minorities, or neurodivergent.
≻ Crucially, all neurotypes, while not equally common, are equally normal.
≻ The scientific fact of neurodiversity is incontrovertible, but its sociopolitical implications are more controversial and currently hampered by wide variability in interpretation and application.
≻ In their paper on the Transdiagnostic Revolution, Astle, Holmes, Kievit and Gathercole present a compelling vision for the widespread adoption of transdiagnostic methods to generate new knowledge which can feed into beneficial practice.
≻ Explicitly combining these scientific arguments with the neurodiversity paradigm can propel us even further towards a science of neurodevelopment that addresses inequality and drives positive societal change.
⚄ Fung, L. K. (Ed.). (2021).
Neurodiversity: From phenomenology to neurobiology and enhancing
technologies.
American Psychiatric Pub.
≻ This book is an introduction to the strengths-based model of neurodiversity (SBMN), designed to integrate and build upon existing theories of positive psychology (Seligman and Csikszentmihalyi 2000), positive psychiatry (Jeste et al. 2015), multiple intelligences (Gardner 1983; Gardner and Hatch 1989), and developmental psychology (Chickering and Reisser 1993) and to apply them to devise strengths-based assessments and interventions for neurodiverse individuals
↩ Main. Top A-C D-F G-K L-O P-S T-Z
⚄ García, C. L., & Vázquez-del-Mercado, A. (2023). Epistemological issues in neurodivergence and atypical cognition: Introduction. Synthese, 201 (5), 147, s11229-023-04100-x. https://doi.org/10.1007/s11229-023-04100-x
⚄ Gobo, G., Campo, E., & Portalupi, E. (2023). A systemic approach to health and disease: The interaction of individuals, medicines, cultures and environments. In A. Pingitore & A. M. Iacono (Eds.), The Patient as a Person (pp. 39–53). Springer International Publishing. https://doi.org/10.1007/978-3-031-23852-9_4
⚄ Grinker, R. R. (2021).
Nobody's normal: How culture created the stigma of mental illness.
National Geographic Books.
≻ We are acknowledging that mental illnesses are more common than we used to think, and that they affect us all – either individually or because of our relationships to others.
≻ Indeed, it is impossible to imagine that there is anyone unconnected to mental illness.
≻ In the twenty-first century, many of the people we most admire celebrities like Lady Gaga and swimmer Michael Phelps, for example – speak publicly about their own emotional struggles.
≻ Stigma isn’t in our biology; it’s in our culture.
≻ It is a process we learn from within our communities, and we can change what we teach.
≻ But only if we know the history of stigma can we target the social forces that created it in the first place, strengthen those that reduce stigma, and say “enough” to the many barriers that keep so many people from getting care.
≻ Not only do scientists know very little about what causes most mental illnesses, mental illnesses are, almost by definition, illnesses without a known cause.
≻ They are patterns of behaviors associated with significant distress or disability in a person’s life.
≻ In the pages that follow, I trace the history of how people with mental illnesses have been judged as abnormal, marginalized, discriminated against, and even experimented on.
≻ Stigma and illness are, of course, very different concepts, but for hundreds of years in Europe and North America mental illnesses have been inextricably bound up with stigma, and so their two histories can be told as one.
≻ We begin at the onset of the industrial revolution, when a march to conformity first begins, and proceed to the present, a time when many mental illnesses and diverse ways of being are less stigmatizing than at any point in our history.
≻ Mental illnesses, we’ll see, are modern phenomena, stigmatized from the moment of their invention.
≻ Another student even wore a T-shirt that read “I hate normal people.” The shirt is a statement of her support of neurodiversity, the movement that argues that neurological and cognitive differences and “deficits,” especially those that characterize autism, are a universal aspect of human variation.
≻ From this perspective, many human differences are pathological or disabling only if society makes them so – like the person in a wheelchair who is “disabled” only when the environment has no ramps or elevators.
≻ In fact, the contemporary term for normal that comes from the neurodiversity movement, “neurotypical,” doesn’t really mean “normal.” It refers, critically, to people who conform to society’s definition of the normal.
⚄ Haegele, J. A., & Hodge, S. (2016). Disability discourse: Overview and critiques of the medical and social models. Quest, 68 (2), 193–206. https://doi.org/10.1080/00336297.2016.1143849
⚄ Harris, Y. R. (2017). The complexities in conceptualizing neurodiversity.
Physics of Life Reviews, 20 , 115–118.
https://doi.org/10.1016/j.plrev.2017.01.020
≻ The neurodiversity movement was launched in the mid-90s with the goals of removing the stigma associated with a diagnosis of autism.
≻ The movement draws from the social model of disability and proponents of the movement argue that rather than conceptualize autism as a disorder or a pathology, autism should be re-conceptualize as a variation in neurological functioning.
≻ The neurodiversity perspective is in stark contrast to the medical model which views disability as “an individual problem tied to functional limitations of the bodies of people with impairments.”
≻ The ultimate goal of the medical model is to cure, manage and treat developmental disorders.
≻ This view dominated much of the scholarship and discourse about the etiology, treatment and outcomes for children and adults with ASD.
≻ Critics maintain the neurodiversity moment only considers those who are “high functioning” and some opponents have argued that the movement is comprised primarily of those from higher socioeconomic status backgrounds.
≻ A second major tension in the field centers on the inconsistent research findings on the social perceptual capabilities of those diagnosed with autism.
≻ While Masataka’s review of the extant literature provides convincing evidence distinguishing the social–cognitive–perceptual differences between neurotypical and neuroatypical children and adults, Weigelt, Koldewyn & Kanwisher contend that there are few qualitative performance differences between children and adults with ASD, and typical children and adults, especially in the area of face identity perception research.
≻ They encourage researchers to continue to determine what factors may drive those existing differences by addressing the following questions.
≻ Are those differences driven by the pervasive allocation of social attention, and or the perception of the social reward system?
≻ Are the deficits in face processing generally true of most people with ASD or are they found in a distinct subgroup of people with ASD and if so how does this group differ cognitively, neurally, and genetically from other individuals with ASD.
≻ I close my commentary with this statement from the Masataka review, which in my opinion frames the clarion call for next steps in the neurodiversity movement in terms of guiding socio-political activism, future research and offering suggestions for teaching and intervention.
≻ “The current review supports the notion that the characteristics of ASD are not an error of nature but an invaluable part of human genetic variability from our deep past, passed down through millions of years of evolution that provide some positive effects for survival advantage.”
≻ I would extend Masataka’s statement to include considerations of culture, broadly and narrowly defined.
≻ Broadly defined subsequent discussions should include considerations of families from culturally diverse communities and narrowly defined discussions should those families from low income backgrounds.
⚄ Heasman, B., & Gillespie, A. (2019). Neurodivergent intersubjectivity: Distinctive features of how autistic people create shared understanding.
Autism, 23 (4), 910-921.
https://doi.org/10.1177/1362361318785172
≻ Intersubjectivity is the process whereby people come together to create understanding (Gillespie and Cornish, 2010).
≻ Building intersubjectivity depends on the social situations, groups, norms and cultures encountered and the creative ways in which people play with imagined perspectives and cultural resources in their everyday sensemaking (Gillespie and Zittoun, 2010).
≻ Intersubjectivity differs from coordination, in that coordination focuses on consensus, whereas intersubjectivity characterises the diversity of ways people create shared understanding.
≻ Studies of intersubjectivity in autism have been primarily based on autistic-to-neurotypical interactions.
≻ These have highlighted difficulties such as shared intentionality (Tomasello et al., 2005) and reciprocating nonverbal cues (García-Pérez et al., 2007; Hobson and Lee, 1998).
≻ However, autistic divergence from the neurotypical norm for interacting (i.e. neurodivergent behaviour) can result in a gap in mutual understanding which makes empathy (Milton, 2012), perspective-taking (Heasman and Gillespie, 2017; Sheppard et al., 2016), and social perception (Sasson et al., 2017; Sasson and Morrison, 2017) difficult for both parties.
≻ This two-way misunderstanding has been termed the 'double empathy problem' (Milton, 2012), and it highlights the dangers of interpreting neurodivergent behaviour on neurotypical terms.
≻ Our findings support previous research on the underrecognised ability of autistic peers to be motivated and able to manage interactions with one another (Brownlow et al., 2015; Ryan and Räisänen, 2008) and highlight the need to examine other contexts for autistic social interactions, particularly given the potential for the activity of gaming to support the features observed.
≻ Thus our findings highlight how neurodivergent intersubjectivity can potentially create rich social interactions.
≻ Certainly, a first step to allowing neurodivergent intersubjectivity to flourish (or at least not be undermined) is to recognise it as having distinctive features that can be enabling.
⚄ Hogan, A. J. (2019). Social and medical models of disability and mental health: Evolution and renewal. Canadian Medical Association Journal, 191 (1), E16–E18. https://doi.org/10.1503/cmaj.181008
⚄ Hughes, J. A. (2021). Does the heterogeneity of autism undermine the neurodiversity paradigm?
Bioethics, 35 (1), 47–60.
https://doi.org/10.1111/bioe.12780
≻ The idea of a neurodiversity ‘perspective’ or ‘paradigm’ has been embraced by many autistic self-advocates and others who consider themselves to be their allies, and is promoted by self-advocacy organizations.
≻ It has, to differing degrees and in different ways, begun to influence more established autism charities and support groups, parents of autistic children, practitioners who work with autistic people, autism researchers, and politicians.
≻ Popular accounts such as Silberman’s
NeuroTribes have brought the idea of neurodiversity to a wider audience and altered public perceptions of autism.
≻ The idea of neurodiversity has also been a subject of fierce controversy.
≻ Some parents of autistic children and parent-led organizations, as well as some autism researchers and some autistic people, have accused neurodiversity advocates of presenting a sanitized view of what autism can be like and deflecting attention and resources away from the struggles of more severely affected individuals and their families.
≻ The term ‘neurodiversity’ is used in various ways.
≻ It can refer to the basic fact of human neurological variation (in much the same way that ‘biodiversity’ refers to the fact of biological variation within an ecosystem), to a social movement aiming to bring about changes in the way societies view and respond to that variation (the ‘neurodiversity movement’), or to particular ways of thinking about the neurological or cognitive differences of which that diversity consists.
≻ The focus of this paper is on the last of these, often referred to as the neurodiversity ‘perspective’ or ‘paradigm’ and understood as a set of claims about autism and other ‘neurodivergent’ conditions, which according to its adherents ‘provides a philosophical foundation for the activism of the Neurodiversity Movement.’
≻ The paper will address one particular challenge to the neurodiversity paradigm that is at the heart of the controversy referred to above.
≻ A difficulty for any discussion of the neurodiversity paradigm is that there is no consensus about what exactly it is.
≻ It was characterized above as a way of thinking about autism and other neurodivergent conditions that is associated with and informs the activism of the neurodiversity movement.
≻ But, as noted by Robert Chapman, whose defence of the paradigm will be considered below, ‘the neurodiversity movement has no leader and no textbook, the arguments and claims its proponents forward are heterogeneous.’
≻ Walker’s account of the neurodiversity paradigm claims that ‘autistics are a minority group, no more intrinsically “disordered” than any ethnic minority.’
≻ Jaarsma and Welin argue that, for the same reasons that homosexuality was declassified as a psychiatric disorder, autism (at least in its ‘high-functioning’ forms) ‘should neither be regarded as a disorder or a disability nor as an undesirable condition per se.’
≻ Ortega refers to neurodiversity advocates who believe that being autistic is like being gay, black or left-handed, in that ‘none are pathological conditions, only ways of being.’
≻ The reasoning implied by such analogies is that, as with homosexuality or membership of an ethnic minority, the only harm or disadvantage associated with autism is that which results from discrimination, and since a disorder is harmful by definition, autism cannot be a disorder.
≻ Supporters of the neurodiversity paradigm understand disability in terms of the social model, according to which impairments, understood as biological or psychological characteristics of individuals, only become disabling in a social context of discrimination or failure to accommodate difference.
≻ As one of the social model’s architects put it: ‘It is not individual limitations, of whatever kind, which are the cause of the problem but society’s failure to provide appropriate services and adequately ensure the needs of disabled people are fully taken into account in its social organisation.’
≻ The claim, then, is that autistic traits are not intrinsically disabling; autism is not a disability in itself, but only in a social context where neurotypical modes of social interaction, communication and behaviour are valued above others, and where those who do not conform are discriminated against or in other ways socially disadvantaged.
≻ A second strand of thinking about neurodiversity focuses on its social value.
≻ This is sometimes expressed by comparing the value of neurodiversity for society with that of biodiversity for an ecosystem.
≻ A third claim that commonly features in academic and non-academic accounts of the neurodiversity paradigm is the claim that autism is ‘natural’ or ‘normal,’ the terms often being used interchangeably.
≻ Walker claims that neurodiversity ‘is a natural and valuable form of human diversity.’
≻ Kapp et al. found that neurodiversity proponents ‘essentialize autism as caused by biological factors and celebrate it as a part of natural human variation.’
≻ For Robison, ‘neurodiversity is the idea that neurological differences like autism and ADHD are the result of normal, natural variation in the human genome.’
≻ It would appear from the discussion in this section that the most central component of the neurodiversity paradigm is the claim that autism (along with other neurodivergent conditions) is not a disorder.
≻ This claim is explicit in influential presentations of the paradigm, and it connects with rhetorical expressions commonly used by neurodiversity advocates, their endorsement of the social model of disability, and their opposition to curative and preventive interventions.
≻ The non-disorder claim is best understood as denying that autism and similar conditions are intrinsically harmful or disadvantageous.
≻ Some parents of autistic children complain that ‘[n]eurodiversity advocates ignore the harsh realities of severe autism, and want to forget about my sons and others like them.’
≻ Neurodiversity advocates may truthfully respond that they campaign for better support for all autistics, not only the more able, but here we must attend to the distinction between the neurodiversity movement and the neurodiversity paradigm.
≻ Even if activists within the movement campaign for all autistics, it may be that views to which many of them subscribe – that autism is not a disorder and that the associated disadvantage is socially caused and is best addressed by social rather than medical means – are unhelpful to some of the most profoundly affected.
≻ The problem for the neurodiversity paradigm highlighted in the previous section is that the non-disorder claim, and more specifically the claim that autism is not intrinsically harmful, cannot be generalized across the autistic landscape.
≻ Autism takes a wide range of differing forms, including some that are reasonably described as mere difference and others where, as Frith puts it, it would seem perverse to deny their debilitating nature.
≻ A second strategy for defending the neurodiversity paradigm against the problem of autism heterogeneity is to argue that the most harmful aspects of autism, those that appear to be suitable candidates for medical treatment and to warrant characterizing autism as a disorder, are not actually part of autism but are co-occurring conditions.
≻ It is often claimed by advocates of the neurodiversity paradigm that autism is a part of an autistic person’s identity.
≻ Chapman, for example, writes of autism and other neurodivergent types as ‘intimately related to the formation and constitution of the self.’
≻ This idea is also apparent in the reasons given by neurodiversity advocates for preferring ‘identity-first’ (‘autistic person’ or ‘autistic’) rather than ‘person-first’ language: autism, it is said, is part of the person, like sex or sexuality, not, like a disorder, a separable (and possibly regrettable) fact about them, so we should no more talk of a ‘person with autism’ than a ‘person with femaleness’ or a ‘person with homosexuality.’
≻ The idea of autism as part of an individual’s identity suggests another way of defending the assertion that autism is not intrinsically harmful.
≻ I have argued that the heterogeneity of autism not only challenges these claims directly but also undermines arguments that are often used to respond to this challenge.
≻ The main focus of this paper has been on the claim that autism is not a disorder but merely a difference, which itself rests on the claim that it is not, in itself, harmful or disabling.
≻ This is the most central of the claims comprising the paradigm in terms of its prominence in the literature and its connections with the practical policy claims that the paradigm is supposed to support.
≻ Rather than denying this or attempting to divide autism into benign and harmful variants, the interests of autistic people may be better served by recognizing that advantages and disadvantages can exist across the autistic landscape and that the magnitude of the latter (and therefore the net effect of a person’s autism) may depend on both intrinsic and/or social factors.
⚄ Jaarsma, P., & Welin, S. (2012). Autism as a natural human variation: Reflections on the claims of the neurodiversity movement.
Health Care Analysis, 20 (1), 20–30.
https://doi.org/10.1007/s10728-011-0169-9
≻ Neurodiversity has remained a controversial concept over the last decade.
≻ In its broadest sense the concept of neurodiversity regards atypical neurological development as a normal human difference.
≻ The neurodiversity claim contains at least two different aspects.
≻ The first aspect is that autism, among other neurological conditions, is first and foremost a natural variation.
≻ The other aspect is about conferring rights and in particular value to the neurodiversity condition, demanding recognition and acceptance.
≻ Autism can be seen as a natural variation on par with for example homosexuality.
≻ The broad version of the neurodiversity claim, covering low-functioning as well as high-functioning autism, is problematic.
≻ Only a narrow conception of neurodiversity, referring exclusively to high-functioning autists, is reasonable.
≻ In its broadest sense the concept of neurodiversity defines all atypical neurological development as a normal human difference that should be tolerated and respected in the same way as other human differences.
≻ In slightly different ways a number of authors suggest that people with different neurological conditions are just different, not handicapped or pathological.
≻ The focus, in the medical model, is upon fixing, curing and correcting deficits and difficulties to enable the individual to live in normal society.
≻ Neurodiversity movement adherents have protested against the medicalisation of the condition now known as Asperger’s Disorder.
≻ Sarah Allred suggests that they should take as an example a successful precedent: the gay rights movement.
≻ The American Psychiatric Association (1973) declared that homosexuality per se was no longer a psychiatric disorder.
≻ In the new outlook on the general concept of a mental disorder it was argued that the consequences of a condition, and not its etiology, determined whether the condition should be considered as a disorder.
≻ Considering the broad conception of neurodiversity, a paradox becomes clear.
≻ If neurodiversity is accepted by society as a special culture, the autists that need care may face a hard time getting it, because their state of being will be regarded as just a natural variation.
≻ The high-functioning autists that do not need care live happily in the knowledge that they are freed from the burden of having a deficit and may have a better life with non interference.
≻ But it may not be so good for low functioning autists or even high-functioning autists that do need care.
⚄ Kapp, S. K. (2019).
Autistic community and the neurodiversity movement: Stories from the
frontline.
Palgrave Macmillan.
≻ This book describes some of the key actions that have defined the autism rights branch of the neurodiversity movement since it organized into a unique community over 20 years ago.
≻ The actions covered are legendary in the autism community and range from “The Autistic Genocide Clock” through to the “Institute for the Study of the Neurologically Typical” and famous pieces of work like
“Don’t Mourn for Us.”
≻ These acts have forged new thinking on autism and established the neurodiversity movement as a key force in promoting social change for autistic people.
≻ It is primarily autistic activists who have been at the vanguard of the neurodiversity movement
⚄ Kapp, S. K., Gillespie-Lynch, K., Sherman, L. E., & Hutman, T. (2013). Deficit, difference, or both? Autism and neurodiversity.
Developmental Psychology, 49 (1), 59–71.
https://doi.org/10.1037/a0028353
≻ This study aims to examine critically this opposition by investigating how awareness of neurodiversity and relationship to autism relate to three potential ways of responding to autism: elimination, amelioration, or celebration.
≻ In apparent alignment with the medical model, many parents of autistic people pursue treatments for their child with the intention of cure, recovery, or at least a more normal appearance
≻ In its pursuit of sociopolitical change and quality of life rather than cure, the neurodiversity movement has drawn controversy over to the extent to which it allows, if not encourages, amelioration of autism.
≻ These findings suggest self-identification as autistic and awareness of neurodiversity reduce neither acknowledgment of deficits associated with autism nor support for ameliorative interventions, while they contribute to viewing autism as a positive identity that needs no cure.
↩ Main. Top A-C D-F G-K L-O P-S T-Z
⚄ Laing, R. D. (1972). The politics of the family and other essays. Vintage Random House. (Original work published 1969)
⚄ Manalili, M. A. R., Pearson, A., Sulik, J., Creechan, L., Elsherif, M., Murkumbi, I., Azevedo, F., Bonnen, K. L., Kim, J. S., Kording, K., Lee, J. J., Obscura, M., Kapp, S. K., Röer, J. P., & Morstead, T. (2023). From puzzle to progress: How engaging with neurodiversity can improve cognitive science.
Cognitive Science, 47 (2).
https://doi.org/10.1111/cogs.13255
≻ Without neurodiversity, cognitive science offers an impoverished account of cognitive diversity.
≻ It dehumanizes neurodivergent communities, and it is missing out on the invaluable contributions of neurodivergent researchers.
⚄ Masataka, N. (2017). Implications of the idea of neurodiversity for understanding the origins of developmental disorders.
Physics of Life Reviews, 20, 85–108.
https://doi.org/10.1016/j.plrev.2016.11.002
≻ The implications of neurodiversity have been most remarkable for education.
≻ The notion has successfully changed the view of intervention with such people, from attempting to overcome what is their weakness to that of enhancing what is their strength: a paradigm shift has occurred.
≻ Rather than putting children into separate disability categories and using outmoded tools and language to work with them, teachers engaging in both special and regular education are able to use tools and language inspired by the ecology movement to diversify learning and assist children to succeed in the classroom.
≻ The current review supports the notion that the characteristics of ASD are not an error of nature but an invaluable part of human genetic variability from ‘our deep past, passed down through millions of years of evolution’ that provide some positive effects for survival advantage.
≻ In addition, there is evidence that humans are provided with an apparently innate attachment for nature and living systems.
≻ Given that this is true for individuals with ASD, and that individuals with ASD appear disabled mainly because they are not adapted for living in modern civilization, it appears to be highly probable that such disabled aspects could be ameliorated by simple forms of exposure to nature such as green environments and pets.
≻ As conservation biology as a science serves as the basis upon which one can secure biodiversity, attempts are needed to synthesize various scientific findings about ASD in order to establish a foundation on which one can argue the importance of maintaining neurodiversity for the future of Homo sapiens.
⚄ McWade, B., Milton, D., & Beresford, P. (2015). Mad studies and neurodiversity: A dialogue.
Disability & Society, 30 (2), 305–309.
https://doi.org/10.1080/09687599.2014.1000512
≻ Those politically aligned with the psychiatric survivor movement tend to reject medical concepts of their distress and as such would not consider themselves to be psychologically impaired, whereas the social model of disability tends to be read as maintaining impairment to be a biological fact (Beresford 2004; Plumb 1994).
≻ Within the neurodiversity movement, all embodied diversity (including neurological differences) is accepted as a facet of human nature, whilst the concept of ‘impairment’ and related purist medical models are commonly denounced as normative (Milton and Lyte 2012).
≻ We need to think collectively about how these processes affect us all.
≻ For example, there are strong resonances here with issues faced by the transgender community who must attain a psychiatric diagnosis and medical certification in order to be recognised as their acquired gender, and who must identify as either male or female and nothing in-between (Hines 2013).
≻ The intersections between neurodiversity and trans* and queer identities are already being realised around the term ‘neuroqueer.’
≻ This term ‘signifies what doctors do to us, it also represents a site of reclamation – to resist both compulsory able-bodiedness and compulsory heterosexuality’
≻ Personalisation has been implemented through a free market ideology that has seen the dispossession and even some deaths of disabled people.
≻ It is ‘time to talk,’ and not in the way the establishment wants us to, with individualised and neatly packaged tales of recovery.
≻ Instead, let us build upon the rich histories of activism and bring our shared experiences of oppression and marginalisation together.
⚄ Meadows, J. (2021, August 12). You're using the word neurodiversity wrong.
Medium. Retrieved March 18, 2023, from
https://jessemeadows.medium.com/youre-using-the-word-neurodiversity-wrong-e579ffa816a8
≻ Discussing autism, ADHD, and dyslexia, this Forbes article claims the term neurodiversity was created to “shift the focus from the negative connotation of these conditions toward the positive,” a statement that waters the entire concept down into a soppy milquetoast version of its former self.
≻ Neurodiversity is a paradigm, a lens through which we look at human neurology, and it stands in opposition to the pathology paradigm.
≻ The pathology paradigm says: there is a normal, healthy brain and an abnormal, unhealthy brain.
≻ People with abnormal brains have something wrong with them and need diagnosis and treatment to become more normal.
≻ The neurodiversity paradigm says: there is no such thing as a normal brain.
≻ Variation in neurology is natural, and none is more right or wrong than another.
≻ The term neurotypical exists as an alternative to the word normal, but it does not describe a type of brain in any biological sense.
≻ It describes a way of being, or a disposition, as scholar Damian Milton says, that is culturally valued and socially advantaged over other dispositions, which we call neurodivergent.
≻ Milton writes: “there is no neuro-typical to deviate from other than an idealised fantastical construction of Galtonian inspired psychological measurement.” (Galtonian referring to Francis Galton, who invented eugenics.)
≻ These terms are sociopolitical, not biological, but everyday I see people making statements like “The neurotypical brain does x” or “
≻ The neurodivergent brain is y”, despite the fact that adhering to the neurodiversity paradigm means acknowledging that there is no biologically neurotypical brain.
≻ A neurodivergent take rejects the normal/abnormal binary altogether.
≻ You can’t be “diagnosed with neurodiversity”, and it is also not a club that admits people based on a list of accepted diagnoses.
≻ There is much clamoring over who “counts” as neurodivergent, but we don’t need to decide which DSM diagnoses count because the entire point of the neurodiversity paradigm is opposing the pathology inherent in DSM diagnoses.
≻ These things are in direct contradiction to each other conceptually.
≻ Being neurodivergent is experiential and political, “a category of power relations and social hierarchisation” as scholar Dieuwertje Dyi Huijg writes in the book,
Neurodiversity Studies.
⚄ Medical model. (2023, March 14). In Wikipedia. https://en.wikipedia.org/wiki/Medical_model
⚄ Ne’eman, A., & Pellicano, E. (2022). Neurodiversity as politics.
Human Development, 66 (2), 149–157.
https://doi.org/10.1159/000524277
≻ The debate around neurodiversity is itself diverse.
≻ As Dwyer (2022) puts it in his own contribution to this special issue of
Human Development, there are multiple “neurodiversity approaches” deployed differently by different actors to different ends, even within the movement.
≻ The neurodiversity movement first emerged in the 1990s as a response to the excesses of traditional autism advocacy.
≻ Though the term would come later, the movement’s origins date back to Sinclair’s (1993) seminal 1993 essay “Don’t Mourn for Us,” encouraging parents to shift their approach to their child’s autism away from cure and towards acceptance.
≻ Sinclair contended that parent-led autism groups encouraged “mourning for what never was” rather than “exploration of what is.”
≻ Sinclair’s immediate predecessors took a very different approach, typically limiting themselves to first-person narrative rather than ethical or political critique.
≻ Autistic authors and public speakers like Temple Grandin spoke predominantly to non-autistic audiences, parents, and professionals.
≻ Though Sinclair engaged in some similar public speaking, “Don’t Mourn for Us” also represented something new: a rebuke of parent autism spaces from an autistic adult, speaking on behalf of a broader community.
≻ When Sinclair wrote that he invited parents “to look at our autism, and look at your grief, from our perspective,” it was the articulation of a larger critique, emerging out of an incipient autistic adult community distinct from the more established and powerful autism parent one.
≻ As other autistic persons responded to the essay and flocked to autistic cultural spaces, this community grew and evolved.
≻ Often, terms that meant one thing to the activists that spawned them have been used very differently by academics and business leaders.
≻ Ambiguity about the “true” meaning of neurodiversity has at times meant that different voices within the movement have sought to confidently present their own views as the only authentic representation.
≻ This ambiguity can also prompt newcomers to adopt and even insist upon positions that would have been alien to or extreme to those who cultivated neurodiversity’s roots (e.g., rejection of autism as a disability or an espousal of unspecified autistic superpowers; see Houting, 2019).
≻ Uncertainty over what the movement stands for has at times prompted observers to attack neurodiversity proponents for views they by and large do not hold.
≻ Much of the present-day debate over neurodiversity is akin to a game of telephone, with many attacking or praising ideas or usages that are very different from what their interlocuters intend.
≻ Inevitable as this may be, discussions of neurodiversity would benefit from awareness of these tensions and the challenges they present.
≻ Neurodiversity proponents would do well to avoid “reinventing the wheel” in a way that might imply a rejection of the broader disability rights movement.
≻ As we shall shortly discuss, there are areas in which neurodiversity ideals add concepts that build upon and are (at the moment) distinct from broader disability rights ideologies.
⚄ Nerenberg, J. (2020).
Divergent mind: Thriving in a world that wasn't designed for you.
HarperOne.
≻ Many people think of outdated, stereotyped images when they consider autism and ADHD, and it’s important to remember that there is a spectrum of experiences.
≻ It’s likely that these labels could apply to people in your own life – perhaps your boss, neighbor, friend, or family member, or even you.
≻ What I see as fundamentally missing from the conversation is a rallying point around diversity in how individuals process sensory input and specifically, recognizing a broad occurrence of heightened sensitivity.
≻ From my research, I discovered that the trait of sensitivity seems almost synonymous with developmental neurodivergences in adult women.
≻ Sensitivity implies a certain heightened reaction to external stimuli experiences, noise, chatter, others’ emotional expression, sound, light, or other environmental changes.
≻ Sensitivity and high empathy are common experiences for many women, but some experience these qualities to more severe degrees, and they remain unaware that they can be hallmarks of Asperger’s, ADHD, HSP, and other traits.
≻ Elaine Aron’s use of the term high sensitivity in her book
The Highly Sensitive Person refers to a person with a characteristic depth of processing of external information – a person with sensory processing sensitivity (SPS), which is the scientific term for HSP.
≻ For someone with Asperger’s, sensitivity might imply a sense of being overwhelmed when overstimulated.
≻ And for someone with ADHD, a common but unknown feature is a sensitivity to one’s own emotions and the regulation of them.
≻ For the person with SPD certain smells or textures heighten their reactions. And for the person with synesthesia (a synesthete), the presence of suffering or strong emotions in others can overwhelm them, an aspect of synesthesia called “mirror touch.”
≻ It is interesting to note that all five of these neurodivergences – HSP, ADHD, autism, SPD, and synesthesia – often imply some version of “melting down” emotionally – adult tantrums, quick appearing migraines, outbursts of anger – because of sensory overload.
≻ Furthermore, how does knowing that neurodivergent people make up at least 20 percent of the population begin to shift our concept of “normal,” “disordered,” or “mentally ill”?
≻ Perhaps we are really talking about humanity as a whole rather than a set of “neurotypical” versus neurodivergent individuals.
≻ Given that so many neurodivergent people go undiagnosed, we may be looking at an entirely different concept of what it means to be human.
≻ Such a shift in understanding could help thousands of women around the world living with undiagnosed or misdiagnosed neurodivergences avoid years of unnecessary comorbidities such as depression, anxiety, shame, guilt, low self-esteem, and distorted self-image.
≻ Neurodiversity, when embraced, can dramatically improve all aspects of life.
⚄ Oliver, M. (2013). The social model of disability: Thirty years on. Disability & Society, 28 (7), 1024–1026. https://doi.org/10.1080/09687599.2013.818773
⚄ Owens, J. (2015). Exploring the critiques of the social model of disability: The transformative possibility of Arendt’s notion of power. Sociology of Health & Illness, 37 (3), 385–403. https://doi.org/10.1111/1467-9566.12199
↩ Main. Top A-C D-F G-K L-O P-S T-Z
⚄ Pellicano, E., & Houting, J. (2022). Annual research review: Shifting from ‘normal science’ to neurodiversity in autism science.
Journal of Child Psychology and Psychiatry, 63 (4), 381–396.
https://doi.org/10.1111/jcpp.13534
≻ The vast majority of autism researchers have been trained to understand autism as a disorder of brain development, an undesirable deviation from the norm.
≻ There have been ‘rumblings’ in autism science, however, of the sort that Kuhn described.
≻ In a context of social change, with many challenges to established power structures, autistic advocates and autism scientists have increasingly called to replace the conventional medical paradigm and consider autism instead through the lens of neurodiversity, where autism is seen as one form of variation within a diversity of minds
≻ The conventional medical paradigm, also known as the medical model of disability (Llewellyn & Hogan, 2000; Marks, 1997), approaches autism as a disability primarily rooted within individuals.
≻ Within the medical paradigm, disability is seen to arise as a direct consequence of a person’s biological make-up and functioning.
≻ The prevalence of deficit-based thinking has the further consequence of focusing attention directly on the individual and away from social and environmental factors that might in fact play a significant role in shaping autistic lives (Engel, 1977).
≻ In the conventional medical view, autism and its associated disabilities are seen as something inherent to the individual.
≻ Taking this individualistic starting point suggests that the ‘fault’ for difficulties in life resides with the individual themselves, thus the burden of ‘correcting’ perceived difficulties lies there too.
≻ The autistic person is perceived to be in some way ‘flawed’ or ‘defective,’ with individual treatment required to remediate these shortcomings.
≻ As well as shaping research findings, this lack of attention to autistic people’s perspectives also has the consequence of ensuring that autistic people themselves have almost no say as to what gets researched in autism science, why or how.
≻ In and of itself, neurodiversity refers to the broad diversity that exists in human neurobiology.
≻ There are countless ways in which the human brain and mind can develop, both structurally and functionally.
≻ Many of these fall within a range that can be considered as ‘typical’ neurodevelopment, while some fall outside of that range and can be considered to ‘diverge’ from the norm
≻ The neurodiversity paradigm refers to a particular set of beliefs and attitudes regarding this diversity (Walker, 2014) and rejects the view that divergence from the norm is a flaw requiring correction This stance can be broken down into two key assumptions.
≻ The first of these is the assumption that typical neurodevelopment is neither superior nor inferior to divergent neurodevelopment.
≻ Neurotypicality does not represent ‘correct’ neurodevelopment any more than English represents the ‘correct’ language to speak
≻ The second key assumption within the neurodiversity paradigm is the belief that even if diversity were not to serve this collective purpose, all people deserve to be treated with dignity and respect, independently of how they diverge from a putative norm, and should be valued for who they are and as they are.
≻ But, fundamentally, those who support neurodiversity accept that a person’s value must not be contingent on their ability to ‘contribute’ to society, economically or otherwise (Kittay, 2017).
≻ As such, the neurodiversity paradigm also broadens the standard understanding of what constitutes a ‘meaningful’ life.
≻ It insists that an autistic person’s life may be rich and fulfilling despite bearing little resemblance to the conventional ideal.
≻ None of this is to suggest, of course, that autistic people do not require supports to enable them to achieve their goals.
≻ The neurodiversity paradigm does, however, lead us to understand the nature of the obstacles that many autistic people face in a fundamentally different way to the conventional medical paradigm.
≻ Neurodiversity is closely aligned with the social model of disability.
≻ Seen this way, any ‘disability’ is not best understood as the result of an individual’s unique characteristics, but rather as a result of an environment that does not effectively accommodate those characteristics
≻ The barriers to autistic people’s flourishing include both those that exist in the physical environment and, perhaps more importantly, social and attitudinal barriers. autistic people must be involved in all decision making that stands to affect autistic people, from the highest levels of policy development to individual support planning; that is, they ‘deserve a full seat at the main table’ first, while the neurodiversity paradigm does not challenge the notion that autism is biological in nature, it stresses the need to view autistic people, not as a collection of ‘deficits’ needing to be ‘fixed’ but as unique and worthwhile individuals, whose lives have meaning and purpose.
≻ It also urges us to look beyond the individual, focusing on (immediate especially, relational – and systemic) contexts and the interaction between contextual and individual factors, to address the negative and disabling effects of being autistic.
≻ Second, while autism science has a strong record of collaborative efforts between academics (Goldstein, Tager-flusberg, & Lee, 2015), including autistic researchers and lay members of the autistic community in these collaborations is still a rare occurrence.
≻ This needs to change. We need to develop far more robust mechanisms of participatory codesign and coproduction in autism research, to ensure that autism science is designed in partnership with autistic people themselves.
≻ Third, once that more participatory spirit does emerge, then we believe autism science will be more likely to focus on autistic community priorities, ensuring that developments in autism science are translated into effective changes in the real-world challenges that autistic people continue to face.
≻ That is, after all, why it matters so much in the first place.
⚄ Pollak, D. (Ed.). (2009).
Neurodiversity in higher education: Positive responses to specific
learning differences.
John Wiley & Sons.
≻ Once we move away from seeing difference as problematic, we can start welcoming diversity as positive enrichment.
≻ Universities have long been havens for neurodiverse individuals, who can find their alternative approaches accepted as tokens of ability rather than markers of deviance, as long as they can survive the rites of passage necessary to graduate and attain higher degrees.
≻ The clichés of ‘absent-minded professors’ and ‘brainy boffins’ unable to manage day-to-day interactions have their origins in the behaviours of highly intelligent, unconventional people who choose to work in contexts where eccentricity is no bar to achievement.
≻ However, the needs of all neurodiverse students need to be recognized and met if we are to provide truly inclusive learning environments.
⚄ Price, D. (2022).
Unmasking autism: Discovering the new faces of neurodiversity. Harmony.
≻ When I use the term masked Autism, I’m referring to any presentation of the disability that deviates from the standard image we see in most diagnostic tools and nearly all media portrayals of Autism.
≻ Usually it’s white boys with conventionally “masculine” interests and hobbies that are flagged as potentially Autistic when they are young.
≻ Even within that relatively privileged class, it’s almost exclusively wealthy and upper-middle-class Autistic kids who get identified.
≻ That group has always been the prototype for Autism when it’s described by clinicians or depicted in media.
≻ All the diagnostic criteria for Autism are based on how it presents in this group.
≻ Every Autistic person is hurt by this narrow conception of the disorder, even the white, rich, cisgender boys who are most likely to be reflected by it.
≻ For far too long, we have been defined only by the “hassle” that white Autistic boys caused their well-off parents.
≻ People with so-called “female Autism” may be able to make eye contact, carry on a conversation, or hide their tics and sensory sensitivities.
≻ They might spend the first few decades of their lives with no idea they’re Autistic at all, believing instead that they’re just shy, or highly sensitive.
≻ In recent years, the public has slowly become familiar with the idea that women with Autism exist, and a few excellent books like Jenara Nerenberg’s
Divergent Mind and Rudy Simone’s
Aspergirls have worked to build awareness of this population.
≻ Not all women with Autism have the “female Autism” subtype.
≻ Plenty of Autistic women visibly self-stimulate, struggle to socialize, and experience meltdowns and shutdowns.
≻ Autistic scientist and activist Temple Grandin is a great example of this.
≻ She speaks in something of a monotone, avoids eye contact, and even as a young child craved sensory stimulation and pressure.
≻ Though she’s very visibly and typically Autistic by today’s standards, Grandin was not diagnosed until adulthood.
≻ Women don’t have “milder” Autism because of their biology; people who are marginalized have their Autism ignored because of their peripheral status in society.
≻ If allistics (non-Autistics) never hear our needs voiced, and never see our struggle, they have no reason to adapt to include us.
≻ We must demand the treatment we deserve, and cease living to placate those who have overlooked us.
≻ Refusing to perform neurotypicality is a revolutionary act of disability justice.
≻ It’s also a radical act of self-love.
≻ But in order for Autistic people to take our masks off and show our real, authentically disabled selves to the world, we first have to feel safe enough to get reacquainted with who we really are.
≻ Developing self-trust and self-compassion is a whole journey unto itself.
≻ >This book is for any person who is neurodiverse (or suspects that they are neurodiverse) and wants to attain new levels of self-acceptance.
≻ Neurodiversity is a wide umbrella, including everyone from Autistics, to ADHDers, to people with Schizophrenia, brain injuries, or Narcissistic Personality Disorder.
≻ This book will outline strategies a masked Autistic person can take to stop hiding their neurodiverse traits, and describe what a world more accepting of neurodiversity might look like.
≻ My hope is that one day, each of us can accept ourselves as the wonderfully weird, mold-breaking individuals we truly are, and live as ourselves, without fear of ostracism or violence.
⚄ Rebecchi, K. (2023, February 6).
Neurodiversity and autism: Between disability and difference, science
and ideology
– Neurodiversité et autisme: entre handicap et différence, science et idéologie.
https://doi.org/10.31234/osf.io/bksxn
≻ The concept of neurodiversity has been developing for more than twenty years under a sociopolitical angle and has since been strongly criticized for its lack of scientificity, the vagueness of its boundaries, the highlighting of a certain conception of autism, the problems linked to intellectual disability, inability to support the theory of a non-disabling difference, and an excessive alignment sometimes with the medical model of disability and sometimes with the social model of disability.
≻ Furthermore, neurodiversity is considered from different angles depending on the discipline and the individual.
≻ The medical model of disability based on a personal problem, the social model of disability based on a societal problem, the neurodiversity mixing innate, acquired, neurodevelopment and psychology in opposition to a norm, and the cognitive diversity highlighting the existence of different cognitions and neurophenotypes outside of psychopathology and the healthy-pathological opposition.
⚄ Reber, D. (2018).
Differently wired: Raising an exceptional child in a conventional world.
Workman Publishing Company.
≻ The übergoal of Differently Wired is to redefine how neurodiversity is perceived in the world, and shift the parenting paradigm to one that acknowledges and includes our experiences.
≻ At its heart, this is a book about saying no – no to trying to fit these squarepeg kids into round holes, no to educational and social systems that don’t respect and support how they move through the world, no to frustration and isolation – and saying yes to the gifts of these unique children and everything that goes along with who they are.
⚄ Reynolds, J. M., & Wieseler, C. (Eds.). (2022). The disability bioethics reader. Routledge.
⚄ Rothstein, A. (2012). Mental disorder or neurodiversity?
New Atlantis: A Journal of Technology & Society, 36, 99–115.
≻ Today, some psychologists, journalists, and advocates explore and celebrate mental differences under the rubric of neurodiversity.
≻ The term encompasses those with Attention Deficit/Hyperactivity Disorder (ADHD), autism, schizophrenia, depression, dyslexia, and other disorders affecting the mind and brain.
≻ People living with these conditions have written books, founded websites, and started groups to explain and praise the personal worlds of those with different neurological "wiring."
≻ The proponents of neurodiversity argue that there are positive aspects to having brains that function differently; many, therefore, prefer that we see these differences simply as differences rather than disorders.
≻ Why, they ask, should what makes them them need to be classified as a disability?
≻ Even if there are special advantages conferred to the depressive mind, it seems problematic, even cruel, to apply the term neurodiversity to those who need intensive therapy and medication simply to live and appreciate living.
≻ For one group of advocates, the move to normalize neurological disorders is a form of gross medical irresponsibility – an ignorant act of cruelty rather than of toleration toward people who are suffering.
≻ When asked whether he would take a pill to cure his autism, Ne'eman replies that "that's an intensely silly question. – predicated on the strange idea that there was or is a normal person somewhere inside me, hidden by autism, and struggling to get out."
≻ This response gets to the heart of the beliefs underlying the neurodiversity movement: these conditions are not simply disorders afflicting otherwise healthy individuals, but are integral parts of who these individuals are.
≻ These advocates hold that the way to address the problems they face is to change the world to make it more inclusive of them and their particular needs, not to change them to fit what the world sees as normal or appropriate.
⚄ Samaha, A. M. (2007). What good is the social model of disability? The University of Chicago Law Review, 74 (4), 1251. https://doi.org/10.2307/20141862
⚄ Shah, P., & Mountain, D. (2007). The medical model is dead – long live the medical model. British Journal of Psychiatry, 191 (5), 375–377. https://doi.org/10.1192/bjp.bp.107.037242
⚄ Shakespeare, T. (2014). The social model of disability. In L. J. Davis, (Ed.). The Disability Studies Reader, (4th ed.), (pp. 214-221). Routledge.
⚄ Silberman, S. (2016).
Neurotribes: The legacy of autism and the future of neurodiversity. National Geographic Books.
≻ The emergence of the concept of neurodiversity: the notion that conditions like autism, dyslexia, and attention-deficit/hyperactivity disorder (ADHD) should be regarded as naturally occurring cognitive variations with distinctive strengths that have contributed to the evolution of technology and culture rather than mere checklists of deficits and dysfunctions.
≻ Though the spectrum model of autism and the concept of neurodiversity are widely believed to be products of our postmodern world, they turn out to be very old ideas, proposed by Hans Asperger in his first public lecture on autism in 1938.
≻ The idea of neurodiversity has inspired the creation of a rapidly growing civil rights movement based on the simple idea that the most astute interpreters of autistic behavior are autistic people themselves rather than their parents or doctors.
≻ Neurodiversity advocates propose that instead of viewing this gift as an error of nature – a puzzle to be solved and eliminated with techniques like prenatal testing and selective abortion – society should regard it as a valuable part of humanity’s genetic legacy while ameliorating the aspects of autism that can be profoundly disabling without adequate forms of support.
≻ They suggest that, instead of investing millions of dollars a year to uncover the causes of autism in the future, we should be helping autistic people and their families live happier, healthier, more productive, and more secure lives in the present.
≻ One way to understand neurodiversity is to think in terms of human operating systems instead of diagnostic labels like dyslexia and ADHD.
≻ The brain is, above all, a marvelously adaptive organism, adept at maximizing its chances of success even in the face of daunting limitations.
≻ Just because a computer is not running Windows doesn’t mean that it’s broken. Not all the features of atypical human operating systems are bugs.
≻ By autistic standards, the “normal” brain is easily distractible, is obsessively social, and suffers from a deficit of attention to detail and routine.
≻ Thus people on the spectrum experience the neurotypical world as relentlessly unpredictable and chaotic, perpetually turned up too loud, and full of people who have little respect for personal space.
≻ Neurodiversity activists have also pushed for more autistic representation in policy making, using the slogan “Nothing about us, without us.”
≻ Fund-raising organizations like Autism Speaks have been resistant to the input of autistic adults, who are arguably in the best position to decide what kinds of research would benefit autistic people and their families most.
≻ “Nothing about us, without us” also extends to the process of doing science itself.
≻ In recent years, a psychiatrist at the University of Montréal, Laurent Mottron, has produced a series of groundbreaking studies on autism with the help of his principal collaborator, an autistic researcher named Michelle Dawson.
⚄ Singer, J. (1998). Odd people in: The birth of community amongst people on the “autistic spectrum”: A personal exploration of a new social movement based on neurological diversity. A thesis presented to the faculty of Humanities and Social Sciences in partial fulfilment of the requirements for the degree of Bachelor of Arts Social Science (Honours), Faculty of Humanities and Social Science, University of Technology, Sydney, 1998.
⚄ Singer, J. (1999). Why can't you be normal for once in your life?: From a 'problem with no name' to a new category of disability. In M. Corker, and S. French, (Eds.).
Disability Discourse (pp. 59-67). Open University Press UK
≻ For me, the key significance of the 'autistic spectrum lies in its call for and anticipation of a politics of neurological diversity, or
‘neurodiversity.’
≻ The 'neurologically different' represent a new addition to the familiar political categories of class/gender/race and will augment the insights of the social model of disability.
≻ The rise of neurodiversity takes postmodern fragmentation one step further.
≻ Just as the postmodern era sees every once too solid belief melt into air, even our most taken-for-granted assumptions – that we all more or less see, feel, touch, hear, smell, and sort information, in more or less the same way (unless visibly disabled) – are being dissolved.
≻ Far from being intimidated, most just indignantly wrote off their GPs, and kept looking.
≻ Whereas the traditional image of ‘diagnosis’ is of something reluctantly sought, dreaded, resisted and imposed from outside, people with ‘marginal’ neurological differences, clamour at the gates, sell-diagnosed, and demanding to be let in.
≻ However, this preference for neurology does not necessarily mean that the medical profession will regain its former exalted pedestal.
≻ Thanks to the Internet, autistics are taking diagnosis, scientific speculation, experimentation with self-medication into their own hands.
≻ News travels fast on the net about what works and what doesn't which practitioners are good and which are not.
≻ With this sense of empowerment, some autistics are in a position to speak with satisfaction about the in about the medical partnerships they have been able to negotiate.
≻ A challenge for the disability rights movement materializes: how do you include people who may need the benefits of inclusion, but cannot bear the physical and emotional presence of it?
≻ The answer from their/our point of view is that we don't want to be included, we want mutual understanding. clear boundaries, appreciation of our gifts, based on what we can do, not what we can't.
≻ Perhaps as the voices of the ‘neurologically different’ are heard more loudly, a more ecological view of society will emerge: one that is more relaxed about different styles of being, that will be content to let each individual find her/his own niche, based on the kinds of mutual recognition that can only arise through an ever-developing sociological, psychological, and now neurological, self-awareness.
⚄ Singer, J. (2017)
NeuroDiversity: The birth of an idea.
https://www.amazon.com/NeuroDiversity-Birth-Idea-Judy-Singer-ebook/dp/B01HY0QTEE/
≻ The lengthy titles of [my] works reflected my eagerness to draw attention to the exciting new perspectives I was discovering from the dawning of a new type of disability, the “Autistic Spectrum Disorders.”
≻ A class of people hitherto marginalized as eccentrics and social outcasts were starting to fight back against the exclusion and mistreatment – from ridicule to active bullying – that had been their lot.
≻ They identified as having a “hardwired” neurological difference, not a personality flaw that was their own fault, nor a psychological problem caused by bad parenting.
≻ And they were about to shake up the existing orthodoxies of not only the medical and psychiatric establishments, but also of the disability rights movements of the era. Since none of the existing disability categories adequately described High-Functioning Autism or Asperger Syndrome, I described them as “disabilities of social communication” in my thesis. The intellectual framework for my thesis was provided by the British-based
Social Model of Disability augmented with the work of American disability theorists.
≻ According to the social model, the experience of disability was socially constructed by society's barriers, negative attitudes and exclusionary practices. Social model theorists opposed what they called the
Medical Model which locates disability in impairments of individual bodies and seeks cures rather than social change.
≻ I will never forget the life-changing phone conversation that confirmed that there was indeed talk of a new, milder kind of autism, called Asperger Syndrome.
≻ And on further reflection, I could see that I, too, had many traits. opened my eyes to the history of disability and how the concept arose as part of the 19th century drive to classify, control and regulate the body, the means by which the “classifiers” gained power at the expense of the “classified” – those people who were unable keep up with demand of the industrial revolution for speedy, efficient and conformist workers.
≻ I learned how the notion of disability served to distinguish between the “worthy” and the “unworthy” poor, and how the distinction continues to function as a means of social control and punishment in our current welfare systems.
≻ I was convinced that Asperger Syndrome was nothing new, and did not believe for a moment that it was caused by vaccination.
≻ I could see that the number of children with Asperger Syndrome at my daughter's schools were no greater than number of “odd kids” in my schooldays.
≻ This word
Neurodiversity did not come out of the blue, but was the culmination of my academic research and a lifetime of personal experiences of exclusion and invalidation as a person struggling in a family affected by a “hidden disability” that neither we nor society recognised for what it was. Nevertheless, we sure knew how to shield ourselves from the critical neurotypical “gaze,” and had developed plenty of strategies to try to pass for normal.
≻ While my focus was on AS, I considered that the scope of neurodiversity was far broader. It could encompass the near-absurdist splinterings of the then DSM IV, even perhaps gender identity and sexual preference, surely properties of the mind.
≻ It seemed to me that the disability rights literature overwhelmingly blamed parents for being willing agents of social oppression by trying to “normalize” their children. And as for “parents,”
≻ I do not think I was being too cynical to read “mothers.”
≻ While this slur never sank to the depths of Bruno Bettelheim's infamous “refrigerator mothers” calumny, nevertheless the age-old remnants of misogyny were evident.
⚄ Singer, J. (2019, October 10).
Neurodivergent from what, exactly? Reflections on the neurodiversity
paradigm.
https://neurodiversity2.blogspot.com/2019/09/question-neurodivergent-from-what.html
≻ Neurodivergent describes the significant percentage of humans who are increasingly recognized as differing cognitively from Neurotypicality.
≻ The adjective neurotypical itself emerged from the Autistic Self-Advocacy movement of the late 20th century.
≻ Pioneers of the movement used it to bypass the increasingly problematic term “Normal,” while essentially pointing to the concept behind it.
≻ It's worth pointing out that the word “neurotypical” should not be read as a diagnostic term, i.e. one that has a specific set of signs and symptoms.
≻ It is purely a term developed to provide a necessary polar opposite of “neurodivergent.”
≻ Neither should the recently coined words based on the concept of Neurodiversity be read as scientific terms.
≻ They are socially constructed terms intended for advocacy purposes.
≻ This should clear up criticisms that these words are “pseudoscientific".
≻ When I first used the word “Neurodiversity,” I did not intend it to be a diagnostic term.
≻ I saw it as a banner for a “Neurodiversity Movement” – a civil rights movement for those of us who had been stigmatized for being “weird, odd, or unfathomable” outsiders.
≻ The adjective neurodivergent became necessary because the adjective neurodiverse is not logically meaningful.
≻ Neurodiversity has been a property of the biosphere since the evolution of sexual reproduction.
≻ It simply says that all human minds on the planet are necessarily different.
≻ So all humans are neurodiverse!
≻ The Neurodiversity Movement is however an identity politics vehicle for people who were discriminated against for differing from the culturally-defined normal range.
≻ There are degrees of difference of course.
≻ Thus “neurodivergence” shades from difference to disability, with a grey area in between.
⚄ Singer, J. (2021, February 21).
Neurodiversity: It's politics, not science! Reflections on the
neurodiversity paradigm.
https://neurodiversity2.blogspot.com/2021/02/neurodiversity-its-political-not.html
≻ I came up with the word “Neurodiversity” for two specific political functions
≻ 1. to add a necessary new category to what is now called “Intersectionality.”
≻ 2. to suggest an umbrella term for an emerging social/political movement based on the pioneering work of the Autistic Self-Advocacy Movement.
≻ It had become clear that ASA movement's paradigm was beginning to be adopted by other Neurotribes who had different diagnostic labels but common issues of exclusion.
≻ The intention was to sound authoritative based on the combined heft of neuroscience and environmental science, not to be scientific.
≻ Take Home Lesson: ND is not a classificatory term dividing us from them.
≻ We are all Neurodiverse.
≻ We live on a Neurodiverse planet in which amoral nature generates endless genetic diversity, while we humans have evolved the capacity to make judgments about nature’s bounty.
≻ What Neurodiversity brings us is a challenge to find a place for everyone and to distribute the bounty fairly.
⚄ Solden, S., & Frank, M. (2019).
A radical guide for women with ADHD: Embrace neurodiversity, live
boldly, and break through barriers.
New Harbinger Publications, Inc.
≻ ADHD women were living like refugees: first, they were marginalized because they didn’t conform to society’s gender role expectations of empathy, organization, and compliance. Second, they were marginalized because they didn’t meet the criteria laid out in the
Diagnostic and Statistical Manual of Mental Disorders.
≻ Too different to measure on society’s yardstick, but not different enough to be permitted the relief of a neurological explanation, women with ADHD were left to attribute their differences to their worst fears.
≻ Invalidated and misunderstood, many internalized the harshest criticisms.
≻ This workbook is intended for women who have attention deficit/hyperactivity disorder (ADHD) and those who help them and love them.
≻ Because we can’t include everything we know about ADHD, this book assumes some familiarity with most ADHD basics.
≻ Our book is called a “radical” guide for women with ADHD to emphasize the simple but “radical” idea that instead of trying to change and fix herself, a woman with ADHD can simply learn to be herself.
≻ This guide is not radical in the sense of promoting any unusual strategies, herbs, or diets, or discarding effective, conventional treatment for the brain-based challenges of ADHD.
≻ To be clear, this book is not anti-medication or anti-strategy.
≻ The ways in which people with brain-based differences are pathologized and compared is similar to how others with more visible differences are judged by a gold standard of the majority. With the concept of neurodiversity, Thomas Armstrong (2010) addresses the much healthier and broader way of celebrating and understanding those with brain-based differences instead of viewing them as inferior.
⚄ Sonuga-Barke, E., & Thapar, A. (2021). The neurodiversity concept: Is it helpful for clinicians and scientists?
The Lancet Psychiatry, 8 (7), 559–561. https://doi.org/10.1016/S2215-0366(21)00167-X
≻ Alongside, but largely independent of evidence-based challenges, has come an ideologically inspired proposal to completely rethink the way we understand these conditions – replacing the notion of disorder underpinned by dysfunction with that of neurodiversity.
≻ Any impairment experienced by neurodiverse people occurs, not as an intrinsic part of a disorder, but because there is a mismatch between their ways of thinking and behaving and their environments.
≻ Their environments are structured in accordance with neurotypical perspectives.
≻ Furthermore, such perspectives can undervalue and undermine the unique gifts, strengths, and qualities that neurodiverse individuals bring to a situation.
≻ By adopting a neurodiversity framework, the researcher will turn the spotlight on the neurodiverse person’s physical and social environment.
≻ They will attempt to understand how the environment’s structure constrains and limits a neurodiverse person and leads to impairment and an undermining of their sense of self and wellbeing.
≻ We eschew a radical interpretation of neurodiversity because a diagnosis and treatment has been shown to be helpful for many.
≻ However, rather than a complete reliance on disorder-based concepts and related treatment approaches, we can see many advantages of incorporating the concept of neurodiversity alongside mainstream research and clinical practice.
⚄ Stenning, A., & Rosqvist, H. B. (2021). Neurodiversity studies: Mapping out possibilities of a new critical paradigm.
Disability & Society, 36 (9), 1532–1537.
https://doi.org/10.1080/09687599.2021.1919503
≻ Neurodiversity is an idea that is much talked about and it has several meanings.
≻ In its most common usage, neurodiversity is used to refer to a supposedly natural variation in the ‘kinds’ of brains in developmental terms akin to biological diversity, which is used to describe the variety of living (nonhuman) creatures (Wilson, 1985).
≻ It is assumed that these brains – labelled as impaired and autistic, ADHD, dyslexic or Tourette’s by psychologists and as ‘neurodivergent’ by activists – conform to categories that reflect the underlying structure of reality as ‘natural kinds,’ which will eventually be confirmed by neuroscientists.
≻ Like biodiversity, the term neurodiversity has come to be used for different purposes, but most often with an assumption that what is natural is always beneficial, which is at odds with the purpose of clinical research that seeks to alleviate suffering.
≻ The problem with this is that it both draws on the ideas of contemporary psychological science without critiquing their conceptual connotations whereby ‘cognitive differences’ are only understood in relation to falling short of an ideal cognitive type, and therefore it does not recognise difference as positive akin to the ecological ideal of biodiversity.
≻ Rather than assume that neurodiversity exists according to the existing clinical categories of autism and related conditions that are discovered by impartial observers, we leave open the possibility that what counts as significant difference between brains should be reconsidered.
≻ This requires reconsidering what it means to be human in the light of contemporary ecological understandings that recognise interdependence rather than the hierarchical divisions of eugenics.
≻ We consider implications of this understanding of neurodiversity for autism research, and propose that we unpick the analogy between neurodiversity and biodiversity.
≻ Comparable to Blume’s discussion of the potentially positive aspects of autism at the expense of difficulties, neurodiversity has been appropriated in employment, social welfare educational paradigms of best practice, where interventions aim at fitting ‘neurodivergent people’ into established hierarchies and ways of doing things.
≻ From this usage, and despite Singer’s advocacy for more diverse understandings, neurodiversity most often serves as a tool for othering neurodivergent students and employees.
≻ We believe that neurodiversity should be understood from a third perspective.
≻≻ This third perspective stems principally from ideas of ‘autistic self-advocacy’ and online communities for the ‘neurodivergent,’ queer or Mad.
≻≻ This perspective focuses, to paraphrase Jim Sinclair’s language, on ‘problems that neurodivergent people have’ rather than the ‘problem we are’ (1992).
≻ While this conception of neurodiversity originates in medical diagnostic procedures, its authority should not depend on clinical recognition or ‘scientific engines of discovery’ (Hacking 2007), and it allows for the possibility of self-diagnosis as equally valid.
≻ Based on the third perspective, we are interested in drawing attention to the cultural construction of normality, particularly in relation to the mind.
≻ In this way, to be neurodivergent simply means to be outside of the category of people who are considered cognitive ‘normal.’
≻ It is a way of being a person that comes from institutional practices of diagnosis and medicalisation but it also involves the production of knowledge about what it means to be particular kind of person.
≻ To be neurodivergent is to reclaim the pathologizing aspects of a long-term cognitive diagnosis and to reclaim one’s neuro-status as a possible position from which to claim resources, representation and recognition.
≻ This suggest that what is needed is a reframing of the medical model so that it no longer necessarily assumes a disordered selfhood. Neurodiversity needs to be connected to theories of justice.
≻ As a result of this, clinicians would need to acknowledge epistemic violence that has been committed in the name of supporting neurodivergent people in the past. To reframe the medical model of neurodivergent conditions, we need to change the ways in which knowledge is produced.
≻ This means changing the epistemic norms. What we are asking for is a new kind of objectivity, which goes further to connect ‘insider’ and ‘outsider’ perspectives on self-knowledge.
≻ It may turn out that what we thought of as authoritative knowledge about other people based on observable behaviour may be nothing of the sort – that our own introspective capacities offer the greatest opportunity for discovery.
≻ Or yet, that neither introspection nor behaviour offer a reliable guide to ‘the bigger picture’ but that the bigger picture becomes clear as we recognise the limitation of our own individual positions.
↩ Main. Top A-C D-F G-K L-O P-S T-Z
⚄ Tisoncik, L. A. (2020), Autistics.org and finding our voices as an activist movement, In S. K. Kapp, (Ed.),
Autistic community and the neurodiversity movement: Stories from the
frontline,
(pp. 65–76), Springer, doi:10.1007/978-981-13-8437-0_5
≻ Though the activism of the 1960s and 1970s had faded, I was still a committed activist.
≻ Activism was no longer a crutch, but an ethical commitment, to right what was wrong and to side with the weak against the predations of the strong.
≻ I was much more content as a human being, much less stressed, though the weird was never far away.
≻ I could answer telephones though I hated them and occasionally destroyed them in frustration.
≻ I even figured out how to get into relationships, more or less, though I had no idea how to sustain one.
≻ Political analysis is about power: understanding who has it, who doesn’t, how the powerful have taken power over others, and how those rendered powerless can reclaim it. Once you learn how to understand injustice in political terms, you cannot help but apply political analysis everywhere you see human suffering.
≻ The skill set works nearly everywhere, because nearly everywhere, when you find a group struggling against disadvantages, you find the same dynamics.
≻ Autistic persons are disadvantaged almost from the moment of birth.
≻ Our power to determine the direction of our lives is taken by presumptions about cognition and perception that simultaneously ignore our abilities and make unreasonable demands upon our disabilities.
≻ We are rejected by our peers, whose bullying is not merely tolerated, but encouraged, by adults, who themselves may join in the bullying.
≻ We are often rejected by our families, and many of us are murdered by them.
≻ We are placed into schools and institutions whose very purpose is to wipe us of our identity, and whose every “treatment” and “care” is an act of violence against who we are.
≻ If we do find work, we are target number one for workplace bullying, and for being fired for autistic traits, regardless of our performance.
≻ We are first to be targeted by criminals and among the first to be targeted by police, at least in the US, where every year unarmed autistic people are among those shot by police, and where autistic people are so often stopped while going about our business we have taken to calling this the crime of “walking while autistic.”
≻ We are more likely to be the victims of violence, yet we are portrayed in the media and by charities “raising awareness” as dangerous perpetrators of violence. Above all we are isolated from society at every stage as the odd, the weird, the other.
⚄ van Grunsven, J. (2020). Perceiving “other” minds: Autism, 4E cognition, and the idea of neurodiversity. Journal of Consciousness Studies, 27 (7-8), 115-143.
⚄ Varela, F. J., Thompson, E., & Rosch, E. (2016). The embodied mind: Cognitive science and human experience. (Revised ed.). MIT Press. (Originally published 1991)
⚄ Walker, N. (2014). What is autism? Neuroqueer: The writings of Dr. Nick Walker. https://neuroqueer.com/what-is-autism/
⚄ Walker, N. (2019). Transformative somatic practices and autistic potentials: An autoethnographic exploration (publication No. 27665905) [Doctoral dissertation, California Institute of Integral Studies]. ProQuest Dissertations and Theses Global.
⚄ Walker, N. (2021).
Neuroqueer heresies. Notes on the neurodiversity paradigm, autistic
empowerment, and postnormal possibilities.
Autonomous Press.
≻ When I first got involved in online autistic communities back in 2003, the word neurodiversity had already been around for a little while.
≻ Very few non-autistic folks had heard of it yet, but autistic rights activists were having some exciting conversations about the word’s implications.
≻ Over the next dozen years or so, through my participation in these conversations and through my published writings, I had the honor of contributing in some small way to the emergence of a new cultural paradigm.
≻ I took to calling it the neurodiversity paradigm, a name which has caught on in some circles.
≻ The autistic rights movement emerged in response to the fact that autism-related discourse and praxis is dominated by what I’ve termed a pathology paradigm, in which autism is framed as a form of medical pathology – a “disorder” or “condition” – and the fact that this pathology paradigm consistently results in autistic people being stigmatized, dehumanized, abused, harmed, and traumatized by professionals and often by their own families.
≻ Just as there are ethnic minority groups and gender minority groups, there are neurocognitive minority groups, and that’s what autistic people are.
≻ By 2010, I’d started referring to these two contrasting paradigms as the pathology paradigm and the neurodiversity paradigm – and in the ongoing conversations within what was now being called the Neurodiversity Movement, I’d begun attempting to articulate the nature of these two paradigms and the core distinctions between them.
≻ The psychiatric establishment that classifies autism as a “disorder”; the “autism charity” that calls autism a “global health crisis”; autism researchers who keep coming up with new theories of “causation”; scientifically illiterate wing nuts who believe that autism is some form of “poisoning”; anyone who speaks of autism using medicalized language like “symptom,” “treatment,” or “epidemic”; the mother who thinks that the best way to help her autistic child is to subject him to Behaviorist “interventions” intended to train him to act like a “normal” child; the “inspiring” autistic celebrity who advises other autistics that the secret to success is to try harder to conform to the social demands of non-autistics all of these groups and individuals are operating within the pathology paradigm, regardless of their intentions or how much they might disagree with one another on various points.
≻ 1. Neurodiversity – the diversity among minds – is a natural, healthy, and valuable form of human diversity.
≻ 2. There is no “normal” or “right” style of human mind, any more than there is one “normal” or “right” ethnicity, gender, or culture.
≻ 3. The social dynamics that manifest in regard to neurodiversity are similar to the social dynamics that manifest in regard to other forms of human diversity (e.g., diversity of race, culture, gender, or sexual orientation).
≻ These dynamics include the dynamics of social power relations – the dynamics of social inequality, privilege, and oppression – as well as the dynamics by which diversity, when embraced, acts as a source of creative potential within a group or society.
≻ The concept of a “normal brain” or a “normal person” has no more objective scientific validity – and serves no better purpose – than the concept of a “master race.”
≻ The neurodiversity paradigm, on the other hand, does not recognize “normal” as a valid concept when it comes to human diversity.
≻ Another useful word is neurominority.
≻ Neurotypicals are the majority; autistic people and dyslexic people are examples of neurominorities.
≻ I’d like to see the term neurominority come into more widespread usage, because there’s a need for it; there are a lot of topics in the discourse on neurodiversity that are much easier to talk about when one has a good, nonpathologizing word for referring to the various groups of people who aren’t neurotypical.
≻ It’s also worth noting that the growing popularity of the term neurodiversity has led to its widespread appropriation as a buzzword by a lot of individuals and organizations who don’t understand its implications and are still very much thinking and operating within the pathology paradigm.
≻ It’s far too common these days to see some website or article that uses the word neurodiversity and then proceeds to talk about autism and/or other forms of neurodivergence in highly pathologizing ways – for example, referring to them as “conditions,” promoting the old pathology paradigm stereotypes and canards, or rating autistic people as “high-functioning” or “lowfunctioning” based on how close they come to passing for neurotypical.
≻ So it’s important to remember that mere adoption of terminology isn’t the same as actually making a meaningful shift in mindset.
≻ What It Means: Neurodiversity is the diversity of human minds, the infinite variation in neurocognitive functioning within our species.
≻ What It Doesn’t Mean: Neurodiversity is a biological fact.
≻ It’s not a perspective, an approach, a belief, a political position, or a paradigm.
≻ That’s the neurodiversity paradigm (see below), not neurodiversity itself.
≻ Neurodiversity is not a political or social activist movement.
≻ That’s the Neurodiversity Movement (see below), not neurodiversity itself.
≻ Neurodiversity is not a trait that any individual possesses or can possess.
≻ When an individual or group of individuals diverges from the dominant societal standards of “normal” neurocognitive functioning, they don’t “have neurodiversity,” they’re neurodivergent (see below).
≻ The neurodiversity paradigm provides a philosophical foundation for the activism of the Neurodiversity Movement, but the two aren’t the same.
≻ The Neurodiversity Movement is a social justice movement that seeks civil rights, equality, respect, and full societal inclusion for the neurodivergent.
≻ Neurodivergent, sometimes abbreviated as ND, means having a mind that functions in ways which diverge significantly from the dominant societal standards of “normal.”
≻ There is no such thing as a “neurodiverse individual.” The correct term is “neurodivergent individual.”
≻ An individual can diverge, but an individual cannot be diverse. a person who is autistic, dyslexic, and epileptic – can be described as multiply neurodivergent.
≻ The terms neurodivergent and neurodivergence were coined in the year 2000 by Kassiane Asasumasu, a multiply neurodivergent neurodiversity activist.
≻ A group of people is neurodiverse [diverse=made up of multiple different types] if one or more members of the group differ substantially from other members, in terms of their neurocognitive functioning.
≻ The opposite of neurotypical is neurodivergent The opposite of neurodiverse would be neurohomogenous
≻ The only appropriate and grammatically correct use of the term neurodiverse is when it’s used to describe a group of people whose members differ neurocognitively from each other.
≻ To describe an autistic, dyslexic, or otherwise neurodivergent person as a “neurodiverse individual” is not merely an incorrect usage of the word “diverse” – it also serves to reinforce an ableist mindset in which neurotypical people are seen as intrinsically separate from the rest of humanity, rather than as just another part of the spectrum of human neurodiversity.
≻ Neurodivergence is a value-neutral term that encompasses any significant divergence from dominant cultural norms of neurocognitive functioning anything from autism to dyslexia to dyspraxia to aphantasia to synesthesia to epilepsy to schizophrenia to PTSD to Williams Syndrome to the cool stuff that long-term meditation practice does to the brains of Buddhist monks.
≻ 1. Never, ever refer to yourself or any other individual as “neurodiverse.” There is no such thing as a “neurodiverse person.” The word you’re looking for is neurodivergent.
≻ 2. Never, ever describe neurodivergent people or neurominority members collectively as “neurodiverse people.”
≻ 3. Never, ever misuse “diverse” as a synonym or euphemism for “member of a marginalized or oppressed group,” whether you’re talking about neurodiversity, ethnic diversity, or any other form of diversity.
≻ The assumption that autism is intrinsically pathological, intrinsically a problem or form of wrongness, leads inevitably to the assumption that the well-being of any given autistic person hinges on that autistic person somehow becoming less autistic.
≻ This in turn has the effect of keeping discourse and praxis focused on eliminating or “treating” autism – using methods that are consistently harmful to autistic people, such as abusive behaviorist approaches or pseudo-biomedical quackery – at the expense of any substantial focus on actions that would actually improve autistic people’s quality of life.
≻ The framework of the neurodiversity paradigm, on the other hand, supports approaches based in the social model of disability.
≻ If we start by recognizing autistic people as a marginalized group, we can see that their disablement is part of their marginalization; i.e., part of how autistics are marginalized within the present social milieu is that their access needs aren’t properly accommodated.
≻ We can also see that the pathology paradigm itself is one of the factors that contributes to autistic disablement – for instance, framing autism as a pathology fosters a societal mindset in which autistic modes of embodiment, expression, and communication are stigmatized as pathological symptoms rather than accommodated. not all neurodivergent people are disabled.
≻ Neurodivergence is a broadly inclusive term that means any significant divergence from dominant cultural norms of neurocognitive functioning.
⚄ Walker, N., & Raymaker, D. M. (2021). Toward a neuroqueer future: An interview with Nick Walker. Autism in Adulthood, 3(1), 5-10. https://doi.org/10.1089/aut.2020.29014.njw
![]()