Note: this file is based upon an OCR rendering of the original text and may contain typographical errors. As well, this OCR has auto-spelling correction (the manuscripts have multiple spelling mistakes). When quoting material please consult the original image files of the text to ensure accuracy. I have tried to maintain a good approximation of the original materials.
Psychoneuroses is not an illness.

By the same author:
Positive Disintegration 1964
(Little, Brown, and Co.)
Personality Shaping through Positive Disintegration 1967
(Little, Brown, and Co.)
Mental Growth through Positive Disintegration 1970
(with A. Kawczak and M. M. Piechowski) (Gryf Publications)
[unnumbered page]
PSYCHONEUROSES IS NOT AN ILLNESS
NEUROSES AND PSYCHONEUROSES FROM THE PERSPECTIVE OF POSITIVE DISINTEGRATION
KAZIMIERZ DĄBROWSKI, M.D., Ph.D.
Professor and Director of Clinical Research and Internship, Department of Psychology, the University of Alberta, Edmonton, Alberta
GRYF PUBLICATIONS LTD.
LONDON 1972
[unnumbered page]
© All copyrights reserved 1972
Printed by Gryf Printers (H. C) Ltd.—171, Battersea Church Rd.,
London, S.W.11. Gt. Britain.
[unnumbered page]
To my wife Ela—Eugenia
the closest companion of my life and work
with deepest thankfulness
[unnumbered page]
ACKNOWLEDGMENTS
I wish to express my deep gratitude to Dr. Thomas Nelson, Chairman of the Department of Psychology, University of Alberta, whose interest and support of my work has been for me a great source of encouragement.
I wish to thank Dr. John Hooz for his work in improving the English of an early version of this book.
Dr. Michael M. Piechowski, whose collaboration I have enjoyed for the past four years, has given me extensive help in rewriting and reorganizing the early version. The reader owes to his nagging and indefatigable criticism a greater amount of illustrative material than originally present. He is also responsible for the tables. The author, alas, has to confess to a tendency to overlook the need for being more explicit.
The Department of Psychology of the University of Alberta is to be thanked for a grant-in-aid which covered part of the publication cost of this book.
I also wish to take this opportunity and express my gratitude to the Canada Council who as a granting agency has made possible a systematic research, now in progress at the University of Alberta, of different levels of emotional and instinctive functions. The concepts of multilevelness of functions first came out of clinical experience and investigation as described here. Various members of my research team, who in a number of ways contributed to the completion of this book, have also been supported by the Canada Council grant.
Mrs. Janice Gordon has enthusiastically typed and re-typed the manuscript a number of times and also expertly carried the load of handling numerous details in making the book ready for the publisher.
K. D.
Edmonton, June 1971
page vi
PREFACE
In this small book I wish to show that so-called nervousness and psychoneuroses are, in most cases, positive developmental phenomena.
In contrast to this writer’s view that psychoneurosis usually represents a phase of accelerated, authentic development, is the opinion, widely held not only by laymen, but also by physicians, psychologists and educators, that psychoneurosis constitutes an illness. But this latter view, we should note, is derived from a consideration of a relatively small proportion of the psychoneuroses, specifically the really serious psychoneurotic syndromes or those which are on the borderline of psychosis as observed in general or psychiatric hospitals or specialized outpatient departments. Close observation, however, of the broad spectrum of so-called psychoneurotic troubles indicates that most forms of psychic overexcitability, anxiety states, depressions, and obsessions, express internal and external conflicts of deep sensitivity which contribute to the development of autonomy, positive maladjustment and existential attitudes. We may even go so far as to affirm that in most cases the milder psychoneuroses, and these are by far the more numerous, comprise basic prophylactic elements which guard a person against sustaining serious mental illness.
Successful treatment of patients is impossible when they are deprived of their own rich, creative endowment and where the possibility of accelerated development is blocked. Hence, “treatment,” in our view, is not properly conceived as “taking away” the psychoneurotic symptoms and dynamisms. Rather, it is understood as the assistance given
page vii
to a person by encouraging and promoting his development and his carrying on the process of autopsychotherapy. Among the principal obligations of the physician, psychologist and educator, then, is to comprehend in each individual case the congeries of positive functions served by the psychoneurotic dynamisms, and to provide conditions conducive to their development. This too involves providing for the development of creativity, which is closely related to the psychoneurotic structures and functions.
In recognizing the positive basis which the complicated developmental dynamisms provide in conjoint function with the so-called pathological dynamisms, the therapist or consultant may assure the psychoneurotic person of his potential for accelerated psychic development, for a currently difficult but ultimately more attractive and authentic way of life.
It is the task of therapy to convince the patient of the developmental potential that is contained in his psychoneurotic processes. Obviously, to achieve that one has to show him this clearly and precisely on the concrete creative and “pathological” dynamisms that are active in his case.
Psychoneurosis does not represent a first phase of mental illness as proposed by Hughlings Jackson (1927). On the contrary, it constitutes the first and necessary phase of positive, accelerated development and contains the germinal seeds of a rich psychic life.
One has to take into consideration that psychoneurotic patients, and the therapists who treat them, are often under the influence of negative traditions and prejudices which have lasted for many years. In the past and now patients are treated as abnormal, strange, maladjusted and ill.
It may be useful to take a look at the source and causes of the traditional viewpoint which regards psychoneurosis as an illness.
1). It seems that we have not adequately clarified and explained the ancient view on psychoneurosis and the borderline of psychosis. The ancient peoples did not pay
page viii
much attention to the strange behaviour of individuals who—apart from their strangeness—displayed an out-standing power of intuition, ability of foresight and prophetic gifts. These individuals were surrounded by general admiration, respect and were under special protection. The prophetic gift was associated with mental overexcitability, a high degree of empathy, ability of concentration and meditation as well as with some forms of the so-called dissociation of personality. On a close examination there can be no doubt that many of the priestesses in famous temples, some of outstanding monks and members of monasteries were psychoneurotic. Socrates, the towering figure of ancient Greece, is actually considered by many experts in psychology and psychiatry as a psychotic and schizophrenic.
2) In the Middle Ages dogmatism and lack of tolerance were widespread if not dominant. In such an atmosphere the very interest in “novelties,” unorthodox ideas, insubordination to and rebellion against precepts grounded on dogmatism, as well as symptoms of oversensitivity, suggestibility, healing with sorcery—any symptoms of mental dissociation—were regarded as evidence of demoniacal possession.
In accordance with the general emphasis on sin and the possession by good or evil spirits it was possible to put on trial alleged witches and people who refused to accept rigid, a priori system of good and evil.
A many-sided, careful analysis shows beyond any question that most of the victims of medieval persecution were psychoneurotic, people endowed with above average independence of mind, creative talent and intuition.
3. The saints were in many ways similar to this group of victims, although, in most cases, they belonged to another level and dimension. They were usually, included in the domain of the “good,” not only because of miracles and their high standard of spiritual life, but also because of their attitude of self-sacrifice and humility, both qualities being absent in the first group. At any, rate, the saints
page ix
were psychoneurotic, and this opinion is confirmed today by outstanding psychologists, and psychiatrists.
It is being contended here that up to our days we have not moved far from the total misinterpretation of psychoneurotic symptoms which prevailed in the Middle Ages. Although we do not believe today in psychoneurotics being possessed by devils, we condescendingly consider psychoneurosis in terms of mental illness, or at least mental instability. This view seems on the surface to be highly humanitarian; it assumes an analogy with somatic illness. The social status of psychoneurotics is “raised” to the rank of sick people. However, it is in fact a denigration; psychoneurotics are still considered something worse than average, something lower, defective, a failure.
The theory of positive disintegration has been presented in detail elsewhere (Dąbrowski, 1964; Dąbrowski, Kawczak, Piechowski, 1970). Since however, we shall be discussing psychoneuroses in the framework of this theory, I have attempted here to introduce different concepts of the theory in relation to clinical material, rather than giving at the beginning a condensed theoretical outline. This should allow the reader to understand the terminology of the theory as applied to the problems, symptoms and syndromes of psychoneuroses discussed herein. In addition, a glossary of terms has been included at the end.
page x
TABLE OF CONTENTS
Acknowledgments — vi
Preface — vii
I. PSYCHONEUROSES FROM THE PERSPECTIVE OF POSITIVE DISINTEGRATION
1. Psychoneurosis as a Process of “Positive” Change of Behavior — 1
2. The Nature of the Psychoneurotic Conflict — 2
3. Psychoneurosis as a Process of Developing a Hierarchy of Values — 3
4. Psychoneurosis as a Growth toward Autonomy — 3
5. The Manifestations of Psychoneurosis and their Social Undesirability — 5
6. The Developmental Potential
(1) Positive development potential
(a) Five forms of psychic overexcitability — 6
(b) Manifestations of the developmental potential in children — 8
(2) The influence of the social milieu on different kinds of the developmental potential — 9
(3) Negative developmental potential — 11
II. FIVE CASES
1. Case 1, W. J — 13
2. Case 2, S. Mz — 26
3. Case 3, S. P — 30
4. Case 4, J. S — 32
5. Case 5, Irene — 35
6. Comparative Analysis of the Five Cases; Unilevel
vs. Multilevel Disintegration — 37
III. NEUROSES AND PSYCHONEUROSES
1. Neuroses and Psychoneuroses as Disorders of Function — 40
2. The Disturbed Function — 43
3. “Arrest” of Development — 43
4. Neuroses and Psychoneuroses: Commonness of Occurrence — 45
5. Classification of Psychoneuroses — 46
xi
IV. PSYCHOSOMATIC CORRELATIONS
1. The Role of Subcortical and Cortical Centers — 49
2. Release of Tension — 50
3. Autonomic Disequilibrium — 52
4. Psychosomatic Disorders — 53
5. Sympathetic and Parasympathetic Tensions — 54
6. Emotions as Disintegrators and Integrators — 55
7. The Etiology and the Level of Psychoneurotic Processes — 56
8. Endocrine Glands — 59
9. Anorexia nervosa — 60
10. Conclusions — 62
V. DISINTEGRATION AND PSYCHONEUROSES IN PERSONALITY DEVELOPMENT
1. Psychoneurotic Traits and Positive Mental Development — 64
(1) Enhanced psychic excitability — 65
(2) Tendency toward more of internal conflict and less of external conflict — 66
(3) Psychosomatic sensitivity as an initial condition of disintegration — 67
(4) Internal conflicts are not subconscious repression
but conscious restructuring of different levels of the psyche — 67
(5) Regression as a purposeful behavior — 68
(6) Positive infantilism — 69
(7) Different levels of fatigue — 71
(8) Quietude and solitude as necessary conditions of psychic synthesis and integration — 72
2. The Role of Polarity in the Process of Positive
Disintegration — 73
VI. PSYCHONEUROTIC SYNDROMES ACCORDING TO THE THEORY OF POSITIVE DISINTEGRATION
1. The Expression of Psychic Overexcitability in Psychoneurotic Processes — 77
(1) Limited developmental potential — 78
(2) Strong developmental potential — 78
(3) Strong developmental potential with marked autonomous dynamisms — 80
2. Case 6, S. M — 82
3. Case 7, Z. S — 85
4. Case 8, M. L — 88
5. Case 9, K. J — 91
xii
6. Hysteria — 93
7. Neurasthenia — 94
8. Psychasthenia — 96
9. Psychoneurotic Depression — 98
10. Psychoneurotic Infantilism — 99
11. Sexual Psychoneurosis — 100
12. Psychosomatic Disorders — 101
VII. INNER PSYCHIC MILIEU IN PSYCHONEUROSES
1. Origin and Development of the Inner Psychic Milieu — 103
(1)Unilevel disintegration — 103
(2)Multilevel disintegration: spontaneous vs. organized — 104
(3) The level of psychoneurotic disorders as a function of the
developmental level of the inner psychic milieu — 105
2. Inter- and Intra-Neurotic Hierarchies of Mental Structures and Functions — 107
3. Levels of Functions in Psychoneurotic Syndromes — 115
(1) Psychasthenia — 116
(2) Psychoneurotic obsession — 118
(3) Psychoneurotic anxiety — 119
(4) Psychoneurotic depression — 121
(5) Hysteria — 123
4. Psychoneurotic Dynamisms as Preventive and Immunological Factors — 124
(1) Psychoneurotic sensitivity — 125
(2) Psychoneurotic “unrealism” — 126
(3) The prophylactic role of depressive and hypomanic states — 127
(4) The prophylactic role of isolation and quietude — 128
(5) The prophylactic role of positive regression — 129
(6) The prophylactic character of different forms of hereditary endowment — 130
(7) Pathological versus psychopathic structures — 134
(8) Summary — 135
VIII. PSYCHONEUROTIC OBSESSIONS
1. The Place of Obsessions in Positive Disintegration — 139
2. Classical Theories of Obsession — 139
3. Clinical Cases of Psychoneurotic Obsessions — 141
(1) Moral obsessions — 141
(2) Obsessions of self-destruction — 141
(3) Ambivalence — 142
(4) Obsessions of death — 144
xiii
4. Obsessive Processes in Creativity — 146
5. Janet’s Classification of Obsessions: A New Interpretation — 147
(1) Examples of sacrilegious obsessions — 147
(2) Obsessions and impulsions of criminal content — 148
(3) Genital and sexual obsessions — 150
(4a) Obsessions of shame in relation to oneself — 150
(4b) Obsessions of shame in relation to one’s body — 151
(5) Hypochondriacal obsessions — 152
6. The Therapy of Psychoneurotic Obsessions — 153
IX. PSYCHONEUROSES AND MENTAL DISORDERS
1. Definition of Psychoneuroses — 154
2. Psychoneuroses and Psychopathy — 154
3. Psychoneuroses and Psychoses — 160
4. Schizoneurosis — 167
5. Psychoneurosis, Paranoia, and Paranoid-like Conditions — 172
6. Psychoneuroses and Mental Retardation — 176
X. PSYCHONEUROSES AND OUTSTANDING INDIVIDUALS
1. Definition of Personality — 180
2. Franz Kafka — 181
3. Gérard de Nerval — 186
4. Jan Wladyslaw Dawid — 190
5. Ludwig Wittgenstein — 193
6. Psychoneurotic Dynamisms and Personality Development — 194
7. The Role of Creative Dynamisms in Psychoneuroses and Types of Development — 197
(1) Creative dynamisms in unilevel and multilevel disintegration — 197
(2) Types of psychoneuroses and types of creative abilities — 199
XI. SUPERIOR ABILITIES AND PSYCHONEUROSES IN
CHILDREN AND YOUNG PEOPLE
1. Methods and Subjects — 202
2. Definition of Some Concepts — 204
3. General Characteristics of the Children Examined and Individual Examples — 205
(1) Case 15 — 207
(2) Case 16 — 208
xiv
4. The Inner Psychic Milieu and the Kinds and Levels
of Psychoneuroses in Young People with Superior Abilities — 211
5. Conclusions — 218
XII. THEORIES OF NEUROSIS AND THEORIES OF DEVELOPMENT
1. Psychoneurosis as a Prelude to Mental Illness — 220
2. Psychoneurosis as an Organic Disorder — 221
3. Regression and Emotional Immaturity as the Source of Psychoneurosis — 221
4. Psychoneurosis as a Disorder of the Reality Function — 222
5. Subconscious and Unconscious vs. Conscious Conflict in the Genesis of Psychoneurosis — 226
6. Adler: Asocial Compensation for Feelings of Inferiority — 231
7. Jung’s Conception of Psychoneurosis and Development — 235
8. Karen Horney: Psychoneurosis as a Childhood Trauma — 243
9. Specific Crises at Successive Stages of Development — 244
10. Lindemann: The Role of Crises in Personality Development — 246
11. Therapist-Client Relationship as a Condition of Growth — 246
12. Psychoneurosis as a Failure of Self-Actualization — 247
13. Psychoneurosis as a Consequence of Guilt — 249
XIII. PSYCHOTHERAPY OF PSYCHONEUROSES
1. Principles — 252
2. Individual Cases and Treatment Programs — 256
(1) Case 17, S. Mo — 260
(2) Case 18, W. K — 265
(3) Case 19, Kristine — 270
(4) Case 20, B. L — 273
(5) Case 21, R. R — 276
(6) Case 22, Barbara — 281
3. Comparison of Psychotherapeutic Programs — 284
GLOSSARY — 289
BIBLIOGRAPHY — 307
INDEX — 313
xv
Be greeted psychoneurotics!
For you see sensitivity in the insensitivity of the world,
uncertainty among the world’s certainties.
For you often feel others as you feel yourselves.
For you feel the anxiety of the world, and
its bottomless narrowness and self-assurance.
For your phobia of washing your hands from the dirt of the world,
for your fear of being locked in the world’s limitations,
for your fear of the absurdity of existence.
For your subtlety in not telling others what you see in them.
For your awkwardness in dealing with practical things, and
for your practicalness in dealing with unknown things,
for your transcendental realism and lack of everyday realism,
for your exclusiveness and fear of losing close friends,
for your creativity and ecstasy,
for your maladjustment to that “which is” and
adjustment to that which “ought to be,”
for your great but unutilized abilities.
For the belated appreciation of the real value of your greatness
which never allows the appreciation of the greatness
of those who will come after you.
For your being treated instead of treating others,
for your heavenly power being forever pushed down by brutal force;
for that which is prescient, unsaid, infinite in you.
For the loneliness and strangeness of your ways.
Be greeted!
xvi
CHAPTER I
PSYCHONEUROSES FROM THE PERSPECTIVE OF
POSITIVE DISINTEGRATION
1. Psychoneurosis as a Process of “Positive” Change of Behavior
The majority of psychopathological conditions, such as nervousness, neuroses and psychoneuroses, are—from the standpoint of the theory of positive disintegration—behavioral patterns of inner, mental changes of a positive character (Dąbrowski, 1964; Dąbrowski, 1967; Dąbrowski, Kawczak and Piechowski, 1970). By “positive” we imply here changes that lead from a lower to a higher (i.e. broader, more controlled and more conscious) level of mental functioning. The process of change may involve mental disharmony, loosening of functions or even mental disorder. Such phenomena as disquietude, astonishment, anxiety, or dissatisfaction with oneself, feelings of inferiority regarding oneself, fear, guilt, certain obsessive or ecstatic conditions, exaggerated control of oneself, strong introvertive tendencies, etc., are processes which often indicate positive changes in building a new inner psychic milieu.
The so-called disturbances of inner feeling (coenesthesia), and dystonia (i.e. disturbances of the autonomic nervous system) may constitute certain primitive requirements giving rise to those conditions which are conducive to self-observation and result in a change of attitude towards oneself.
A profound knowledge of oneself and a deep level of emotional experience, as well as a more meaningful contact with the environment seems to be impossible without going through conflicts, disharmony, intensified sensitivity, and even organ-
1
is or mental illness. While it is true that certain internal somatic or neurological disturbances exhibit symptoms similar to psychoneurotic symptoms, there are as yet no sufficient grounds for deducing a somatic etiology in psychoneurosis in general. In our opinion the latter view is an erroneous oversimplification. The tendency to treat psychoneuroses as being symptomatic of the first phase of a more serious mental disease as postulated by Jackson (1958) and supported by other authors (Sargent and Slater, 1954)—can no longer be maintained.
2. The Nature o f the Psychoneurotic Conflict
A great majority of Psychoneuroses represent “positive disorders”; they are psychogenetic (i.e. originating in the psyche), and are often expressive of rich personality nuclei in individuals capable of developmental, even accelerated, change. They are expressive of conflict between an inner personal milieu, and the outer milieu, precisely because they exhibit tendencies towards a concern for that which “ought to be” instead of adjustment to that “which is.”
Psychoneuroses are observed in people possessing special talents, sensitivity, and creative capacities; they are common among outstanding people. Psychoneurotic syndromes are not found among those who are moderately or considerably mentally retarded. With all due regard to present general medical, neurological or endocrinological methods of treatment, in our opinion it is essential that psychologists and psychiatrists do not reduce Psychoneuroses to organic factors. Rather it is our main task to understand them as representing an individual complex evolution of conflicts. These conflicts yield positive effects, i.e. their outcome is individual growth, and it is our task to see also their other aspect, i.e. as difficulties in contact with the environment, or opposition to pt, when invariably it is the psychoneurotic individual that is morally superior to his environment, and therefore cannot adjust to it. Thus we find both inner and outer collisions in individuals who are characterized by constitutional elements of positive or even accelerated development.
2
Psychoneuroses should be approached from both psychological and neurological viewpoints in regard to their etiology, pathogenesis, diagnosis, and therapy. This is already evident from the mere consideration of the meaning of the term itself: psychoneurosis. Furthermore it is necessary to ask what developmental functions are involved. What protective mechanisms have appeared in connection with these “disorders,” in both the inner and outer milieus. What values have been shaken in their hierarchy, and what have been the attempts of the individual to recover them, or to exchange them for higher or lower values.
3. Psychoneurosis as a Process of Developing a Hierarchy of Values
“Psychoneurotic experiences” by disturbing the lower levels of values help gradually to enter higher levels of values, i.e. the level of higher emotions. These emotions becoming conscious and ever more strongly experienced begin to direct our behaviour and bring it to a higher level. In this way higher emotions play a dynamic role in our development and give meaning to our life. As new and higher values the higher emotions slowly begin to shape our “new harmony” after the collapse of the primitive harmony of lower level. The problem of value is essential and emerges sooner or later in each case of psychoneurosis.
The problem of the meaning of life and of authentic thinking and feeling is also common and outstanding. Hence the psychoneurotic problem is one of the lack of adjustment manifesting protest against actual reality, and the need for adjustment to hierarchy of higher values: to adjust to that which “ought to be.”
4. Psychoneurosis as a Growth toward Autonomy
The feelings of internal discard (subject-object in oneself, feelings of dissatisfaction with oneself and guilt, are common experiences in life. Guilt feelings here do not stem from a repressing action of the “superego”; neither do they have to be an
3
expression of real guilt of the psychoneurotic patient. They indicate rather an excessive sensitivity to the inner milieu, in which there appears, concomitant with a tendency for accelerated development, a sense of inferiority in relation to oneself, a feeling of having “wasted” one’s possibilities for fulfillment, of having betrayed one’s ideal, and an exaggerated perhaps sense of personal responsibility. Hypersensitivity—whether internal or external—may be, and often is, out of proportion to the real guilt.
Psychoneuroses—especially those of a higher level—provide an opportunity to “take one’s life in one’s own hands.” They are expressive of a drive for psychic autonomy, especially moral autonomy, through transformation of a more or less primitively integrated structure. This is a process in which the individual himself becomes an active agent in his disintegration, and even breakdown. Thus the person finds a “cure” for himself, not in the sense of a rehabilitation but rather in the sense of reaching a higher level than the one at which he was prior to disintegration. This occurs through a process of an education of oneself and of an inner psychic transformation. One of the main mechanisms of this process is a continual sense of looking into oneself as if from outside, followed by a conscious affirmation or negation of conditions and values in both the internal and external environments. Through this constant creation of himself, through the development of the inner psychic milieu, and development of discriminating power with respect to both the inner and outer milieus—an individual goes through ever higher levels of “neuroses” and at the same time through ever higher levels of universal development of his personality.
In order to better understand this approach and to see it realized, an attitude needs to be developed among doctors, among patients themselves, and among those affecting their environment, that “patients,” rather than being manifestly “cured,” should be provided with conditions conducive to their development. Psychoneurotics, rather than being treated as ill, should be considered as individuals most prone to a positive and even accelerated psychic development.
4
Restoration or re-elaboration at a higher level of a patient’s personality is the postulate of existential psychotherapy (May, 1961; Laing, 1965, Frankl, 1967), of “integrity therapy” (O. H. Mowrer’s psychotherapy which allows the integration of personality through sincere and open “confession of guilt” in a psychotherapeutic group, Mowrer, 1964), and the theory of positive disintegration, although in each case expressed differently.
5. The Manifestations of Psychoneurosis and their Social Undesirability
The terms neurosis and psychoneuroses are used every day. It is common in industrial settings to ascribe work absenteeism to such reasons. The general practitioner is quite familiar with this problem. When the physician cannot find organic changes underlying various subjectively unpleasant experiences of daily life, personal difficulties, bad feelings or various symptoms, they are then attributed to neuroses.
All states which appear to be unwarranted by existing external conditions, such as: anxiety, states of nervousness (i.e. increased psychic sensitivity), obsessive thoughts related to an apparent danger for us or for our children, intense emotional fatigue or depression, “nervous sleep,” hypersensitivity, an increase in rate and strength of heart beat, etc., are universally considered by a majority of physicians, specialists or not, as manifestations of neuroses or psychoneuroses.
On the one hand there is a general—and largely correct conviction—that neuroses and psychoneuroses are not grave conditions, and do not lead to the dissolution of mental functions. In most cases they still permit the continuation of one’s work, albeit less effectively. On the other hand it must be recognized that they are a nuisance, cause fatigue, weaken one’s positive approach to life, etc. They prohibit or limit a pleasurable outlay of energy, they weaken or close—at least periodically—a proper contact with our environment, and cause much difficulty in both our home and professional lives. We know that during various
5
social changes or upheavals, such as post-war periods of great tensions and instability, the number of disorders of this kind increases considerably. A social security report from Zurich shows that less than ten years after the Second World War about 70 percent of all patients were cases of neurosis or psychoneurosis (Brun, 1954), Similar percentages are found in out-patient clinics in England, France, Poland and other countries while in the United States only 20 percent of the people were found to be free of signs of emotional distress (Srole, Langer, Michael, Opler, and Rennie, 1962), and one third of a small town population was found to have distressing psychiatric symptomatology (Leighton, 1956).
What is the basis of these disorders, what are their causes, their development and their outcome? We shall try to give an answer in the pages to come. We shall also try, as already indicated, to shed some light on the positive correlation between accelerated development, creative tendencies—and neuropsychic complexes.
Before presenting some clinical material we have to introduce the concept of the developmental potential.
6. The Developmental Potential
In the great majority of cases of psychoneurotic “constitution” the author sees present, more or less clearly, nuclei of a positive developmental potential. In many cases this potential is of the kind that predisposes the individual for an accelerated development, for the development of his talents, or for the development of an eminent personality.
It is our opinion based on extensive experience that there is never, or almost never, a case of accelerated development, and even more so of eminent development, without a psychoneurotic constitution.
(1) Positive developmental potential.
(a) Five forms of psychic overexcitability.
The main form of the positive developmental potential are five kinds of psychic overexcitability namely, sensual, psycho-
6
motor, affective (emotional), imaginational and intellectual. Each form of overexcitability points to a higher than average sensitivity of its receptors. As a result a person endowed with different forms of overexcitability reacts with surprise, puzzlement to many things, he collides with things, persons and events, which in turn brings him astonishment and disquietude. One could say that one who manifests a given form of overexcitability, and especially one who manifests several forms of overexcitability, sees reality in a different, stronger and more multisided manner. Reality for such an individual ceases to be indifferent but affects him deeply and leaves long-lasting impressions. Enhanced excitability is thus a means for more frequent interactions and a wider range of experiencing.
An individual who is excessively sensitive sensually possesses a more or less superficial sensitivity to beauty, is suggestible, is more exposed to the difficulties of life. An individual who is psychomotorically overexcitable is restless, curious, cannot sit still in one place, wanders around, has an insatiable need of change and of “wandering into space.” An individual who is emotionally overexcitable is sensitive, takes everything to heart„ is syntonic and even more often empathic though not necessarily in a highly developed manner. He has a need of exclusive and lasting relationships, of help and protection, of understanding suffering. An individual who is overexcitable in respect to imagination is sensitive toward “imaginational realities,” is usually creative, has vivid fantasy and is often full of ideas and plans. He displays abilities in poetry, art or music. He has his “kingdom of dreams and fantasy.” An individual intellectually overexcitable shows strong interests early in inner and in external life, has strong nuclei of analysis and synthesis. Early in life he is capable of asking questions and demanding logical answers.
Some forms of overexcitability constitute a richer developmental potential than others. Emotional (affective), imaginational and intellectual overexcitability are the richer forms. If they appear together they give rich possibilities of development and creativity. If these three forms of overexcitability are combined with the sensual and psychomotoric then these latter two are
7
both enriched and enhanced in their positive developmental possibilities.
(b) Manifestations of the developmental potential in children.
Almost all these forms of overexcitability can be detected between 1 and 2 years of age and the older the child the more they are discernible. We can note these potentials in an excessive and global mobility of the child, in its sensitivity to colours, sounds, tastes, smells, in its need for affection, fondling, in silent moods, early sadness and spontaneous joy, in early syntony—even empathy—far parents and siblings, in richness of observation, in quick penetration into the world of fantasy and imagination, in early reflection about himself, about life and about death. Such reflections can appear already in children 3-4 years, old. For instance, one four-year-old girl said. “Death is a trip but it is hard to get out of the hole in the ground where they put the dead person.” The same girl also asked: “How can you tell whether someone is sleeping or dead?” Another five-year-old girl created for herself whole new realms of existence with leprechauns, birds, squirrels. The door to the attic was the door to these realms which appeared to have a character of sacred mysteries.
Developmental potential can also be observed in children in connection with strong special interests and abilities. If a child has enhanced intellectual excitability then at the age of asking questions he will not be satisfied with automatic answers but will ask a second and a third time, often forming the questions in a new way as a result of new associations. Some children are surprising by their perceptiveness of the world around them, by their childish “philosophical” outlook. Some children show early mathematical abilities in relation to mathematical-philosophical and magical problems.
There is a great number of children who at the age of 4-6 write poetry distinguished by deep content and good form. One six-year-old girl when asked by her mother whether she did not get tired by dancing so often answered: “Mother, I don’t get tired because I don’t dance, it’s only my feet who do the
8
dancing.” In this expression we can see besides a marked refinement of thought, a nucleus of the development of the inner psychic milieu, initial forms of the dynamism “subject-object in oneself” and a developmentally significant dualistic attitude (a manifestation of different levels of experience).
These nuclei of the inner psychic milieu together with psychoneurotic elements appear in the feeling of shame, which is much stronger than usual, in the feeling of guilt when the child has caused sorrow, and in a desire to make good. In such experiences there is frequently hidden the germ of an ideal which in its main outline the child has developed on its own, whether with the support of, or against, its environment. Quite often the child shows some dissatisfaction with himself and is feeling different from what he thought he was and what his parents thought he was. Here is the beginning of an interaction between the developmental potential and the influence of the environment.
A separate group of the nuclei of the developmental potential (although not strictly isolated from the above) are traits which later in life are called neurotic. Such is for example an excessively strong exclusivity of attachment to close persons, fear of their falling ill, longing for their return when they are away. Such are for instance phobias of contact with certain animals like earthworms, lizards or snakes; phobias of dirty water, unknown situations in the environment, possibility of disappointment, and symptoms of neurotic expectation, etc.
(2) The influence of the social milieu on different kinds of the developmental potential.
It goes without saying that the constitutional nuclei are highly modulated positively or negatively by the social milieu.
When the developmental potential is very strong and very rich even a negatively acting social milieu is of secondary importance. If the nuclei of the developmental potential are weak, or if they also contain some negative components then the character of the social milieu is of decisive significance. If it is nourishing then individual growth will be supported where
9
it is lacking in its natural endowment, if it is negative then severe pathology is most likely. If the developmental potential has distinctly negative character then the influence of the social milieu is without much significance.
Besides the constitutional endowment expressed as nuclei of the developmental potential and the influence of the social milieu there is a third category of forces that is very important in the shaping of psychoneurotic processes. These are the autonomous factors which develop gradually throughout the individual’s life experiences. Becoming more and more conscious they often come to play the most important role in the evolution of psychoneurosis as a growth towards autonomy and self-determination. These autonomous factors find their expression in education of oneself, in autopsychotherapy, and in richer use of the individual’s creative abilities.
In individuals whose developmental potential is more limited and who also present low psychic resilience because their developmental nuclei are somewhat weak, the stereotyped social influence reduces their abilities for creativity for the sake of adjustment and may lead to negative disintegration. In individuals who are richly endowed and talented the same influence leads to psychoneurotic creative processes which, although rich in their content, are described by the social milieu and the physicians as pathological. Such a label is, of course, detrimental to both the psychoneurotic individuals and the society. In this, way the path of collisions between psychoneurotics with their creative components and the environment takes shape. The path of these collisions is a hard road of liberation for creative individuals, it is a path of suffering—not always necessary and not always useful. It is a path which does not quickly lead to finding one’s own road of development because of the strong inhibitions and frequently high suggestibility of these individuals.
These different forms of the psychoneurotic developmental potential constitute in their totality the “royal path” of hierarchical development—through multilevel disintegration, inner conflicts, creative instinct and instinct of self-perfection—toward secondary
10
integration, i.e. toward the united, harmonious and highest spiritual reality which is liberated from lower levels of the unconscious and in which one experiences contents previously known consciously but only intellectually (i.e. without the dynamic participation of higher emotions).
(3) Negative developmental potential.
In a significant number of cases of isolated forms of sensual or psychomotor overexcitability (i.e. when there is no admixture of other forms of overexcitability), in cases when the nuclei of the inner psychic milieu, wider interests and abilities, and sharp awareness of one’s own developmental path are lacking, we are dealing with a negative potential which is not helped by the influence of the environment, but on the contrary, is harmed by it.
It is difficult to speak of a negative psychoneurotic potential because a negative developmental potential covers the borderline of psychoneurotic nuclei, psychopathy, psychosis and even mental retardation. When enhanced psychomotor and sensual overexcitability is combined with strong ambitions, tendencies to showing off and lying, it constitutes a nucleus of psychopathy with some neuropathic components. This is a potential for the development of characteropathy, or, better, of hysterical psychopathy.
Tendencies toward disintegration with very limited or quite absent activity of the developmental instinct, and with a greater strength and number of disintegrating dynamisms over the integrating ones, are found in the potential on the borderline of psychoneurosis and psychosis. On the borderline of mental retardation and psychoneurosis (or, rather, neurosis) the developmental dynamisms appear weak pointing to a very limited developmental potential.
These forms of the developmental potential—insufficient for positive development—may be called abiotrophic to denote the absence or degeneration of the normal functions of the organism, in this case as applied to mental development.
11
We can summarize as follows
(1) The presence of neurotic or psychoneurotic positive developmental potential guarantees creative development through higher forms of psychoneurotic processes such as internal conflicts, hierarchization, development of autonomous and authentic dynamisms, towards a high level of personality and secondary integration,
(2) Developmental potential which is not universal and of weak tension may lead either to positive development through nervousness and psychoneuroses, or to negative disintegration, psychosis or suicide. The environmental influence is to a very great degree responsible for the path which will be taken.
(3) A separate obstacle for both groups of individuals with developmental potential either (1) or (2) is the established attitude of society, when physicians and psychologists treat psychoneurotics as abnormal, and worst of all—sick. This attitude is primarily responsible for inhibition, isolation, noncreative feeling of inferiority and lack of a creative and rich development. These conditions create collisions between their creative inclinations timidity, and lack of self-confidence; they create the loneliness of psychoneurotics.
12
CHAPTER 11
FIVE CASES
The following discussion of several clinical cases is intended to give the reader an introductory orientation as to the kind of neurotic disorders characteristic of the processes of positive disintegration as well as to the manner of interpretation and diagnosis. This will serve as a basis for psychotherapy based on the theory of positive disintegration.
Case 1
W.J. was a young housewife approximately 30 years old. When she came for therapy I asked her to write in some length her life history, which she did submitting a manuscript 35 pages long. She had no important history of pathological hereditary endowment, since neither her parents nor her grand-parents and other close relatives suffered from psychosis, mental retardation or psychopathy. She had a happy early childhood, a quiet home, care and love of her parents, which contributed to her feelings of security. As a child she believed that her mother was able to deal with any potential danger. The patient had still greater respect for her father and avoided offending, him in any way. From early childhood she was shy and although she never had bad experiences with animals, she was afraid of them, especially dogs and cats. She was afraid of being bitten by a dog, being kicked by a horse, or being attacked by a cow.
She said that even as a child she was an egoist. If she had something to share with her younger sister, she used to take the larger part. When she went with her father, brother, and
13
sister for a sleigh ride, she wanted her brother to go first, and only when he came out safely would she then go herself. She writes that she was never a joyful child, but was rather inclined to emotional reactions, melancholy and sorrow. Further she says that when she was only 5 years old, one of the elder boys asked her mother why she always had such a sour look on her face.
In spite of her statement as to her lack of a joyful attitude, the patient maintained that she took pleasure in playing with other children. But this joy was often stifled through excessive caution or fear of falling down, bumping into something, or bringing some calamity upon herself. She was very much aware of her sister’s several minor accidents while playing and the subsequent anxiety at home, doctor’s visits, treatment, etc. When she was six years old her first encounter with an accident left on her very strong impression. She saw an ambulance and a woman lying on a litter covered with something white. She vomited at the sight and then fainted. Later she always experienced nausea following an emotional upheaval.
The patient also had considerable trouble in facing new situations. She did not want to go to kindergarten; then while going to school she became excited and cried spasmodically. She had no sense of duty in the preparation of her lessons, so she often played all day. Only in the evening did she make up her lessons. When her parents once decided to give her no help in their preparation, she stayed up till 11 o'clock at night, cried during the lesson, and thought of various punishments for her parents, including her own death.
All these unhappy events and physical reactions promoted an attitude of anxiety. She felt strong anxiety regarding the fate of her parents, especially her mother. When she was seven she felt deeply concerned about her mother’s surgical operation, even though it was a mild case and was performed in an outpatient clinic. At that time she lied cross-like on the floor and prayed very long for a successful operation. At another time she had a shocking experience when her father had a heart attack and lost consciousness. She was frightened, went pale and trembled all over. However, when facing an accident, she could at times con-
14
trol her feelings to the extent of participating in caring for the wounded. At the age of 10 or 11, when her mother was absent she prayed ardently for her happy return. During the time of her mother’s absence, she took her mother’s nightshirt to bed since she somehow felt better that way.
At ten she had scarlet fever and tried to extend for as long as possible the convalescent period at home because here she felt most secure. Following this sickness she went to school but suffered from anxiety and feelings of insecurity. She changed her grade school several times without evident reason. Each time the school she attended became unpleasant or obnoxious to her, she asked her parents to transfer her to another school under such pretexts as needing a location closer to home, higher standard of learning, etc.
She liked very much to participate in a school theatre or play with other children in the backyard. Usually she assumed the function of an impresario and played a male role. She wrote literary scenarios based on fairy tales. Those artistic activities gave her much joy; she also wrote verses and novels, and dreamt that some day she would see her books on library shelves.
She deeply felt the period of the uprising.* Her reaction to those events often included vomiting. About that time, too, she witnessed her father’s arrest by the Germans. Following a moment of stupor she ran screaming towards her father and the German patrol, and felt like throwing herself on them in defense of her father, but did not. One may note here that when her altruistic feelings (concern for her father) reach very high tension then her whole psyche becomes well organized. This points to distinct developmental possibilities.
She was terrified when she found herself, accidentally, in the front line of battle facing bombings, wounds, and death. In recalling those events after several years, she trembled nervously. Passing from the knowledge of an approaching imminent
_____________________
*The Warsaw uprising of 1944, when most of the city was destroyed.
15
danger (house searches by Gestapo, arrests of neighbours and the like) to the realization that the whole family was safe, she got a fever.
While attending high school she tried to look more mature than she was in order to capture the attention of her elder colleagues. At this time she used to write for a school paper and participated in a school theatre. This was a very enjoyable period for her. She belonged to girl-guides but avoided going to camps, for she was afraid to leave the home milieu.
She was strongly aroused emotionally during flirtation, and her first kiss left her unconscious. She was rather infantile and at that time no further physical contacts were made. Following this event she looked upon herself as a mature woman, but had guilt feelings in relation to her mother who had impressed strong moral principles upon her. That evening she dreamt of an ideal boy—a husband—she imagined a beautiful house, marriage, nice children, and that she was madly in love with her husband. At this time, she had outbursts of anger, crying, and periodic anxiety with momentary numbness of the hands. During this time, too, she was supposed to take part in a show, in a solo scene, but she panicked and refused to play the part.
At one time she became weak during a lecture-twice in the same day. Physicians directed her to take tests, and she went through them with anxiety. She felt ill all day before the tests, and at night she rose up with a cry and took to the corridor. She felt that she was falling down and saw her mother as if from very far. After this event, which she called “an attack,” she experienced trembling of her whole body. This event also aroused new forms of anxieties, especially in connection with the possibility of a repetition of the attack. So she did not want to leave home, and she stopped going to school. For many weeks she appeared very weak. She then had another attack of this kind, but much milder.
At that time she was seen by many physicians. She stayed in bed a long time, and when she tried to get up, experienced dizziness and tingling in the feet; so she no longer got up.
16
Numerous clinical tests were made. She received injections of neurotonine (a medicine for toning up the nervous system). Still the fears did not dissipate and she never went out by herself. She kept away from school for fear of another “attack.”
Following some weeks of rest her condition was improved and she resumed going to school. However, she awaited the end of every lesson with trembling. She went from physician to physician seeking a remedy. Finally on a neurologist’s advice she was placed in a ward for neurotic patients. After psychotherapeutic and tranquilizing treatment her strong fears were dissipated, but she developed, she said, a fear of a mental disease. She maintained that she found shock treatment very hard to bear and had very strange feelings during that treatment. Specifically she did not like to see herself in a mirror. She was constantly afraid of becoming mentally ill. Following her return to school, she again became afraid of an oncoming “attack.” But these fears were now less severe. The patient again intended to stop her school attendance, but during these periods of doubts there appeared new circumstances. She found compatible associates and engaged in sports. This gave her considerable self-assurance; she found an outlet in skating and ball games.
At that time she fell in love which greatly absorbed her. She was 18, it was a good year. Conditions at home were good; she was well liked at school; she worked socially, and was in love. Once, however, she fell ill with influenza, after which she felt bad again, and felt overworked because of her approaching graduation from high school and excess of social activities (school drama in particular). She then experienced a very strong feeling of estrangement. Although feeling ill, she still prepared for finals and passed very well. Immediately after, she took insulin treatment at a local clinic and this had a favorable effect on her general well-being. Later she entered into a sexual relation with her fiancé which gave her much pleasure, but she was physically disappointed mainly due to her inability to reach an orgasm. She loved her fiancé, respected him highly, but at the same time had pangs of conscience towards her
17
mother who did not suspect that she was living with him. During this period she felt better, then again worse, and was almost constantly bothered by feelings of estrangement of varying intensity. About that time she married her fiancé. Rather soon, however, she met someone else for whom she felt an emotional attraction, and the attraction was mutual. Still, moral bonds did not permit any rapprochement. At this time, most fears disappeared for as much as a four year period. In this period of her life moments of great joy and general satisfaction acted as a force that pulled her together and subordinated her disintegration to constructive trends.
Both her continued studies and those of her husband did not allow them to live together. During this time the patient became pregnant. New conditions, independent professional work, and living with her husband in a new home of their own gave her much joy. She became satisfied with life. Her one worry was being away from her parents. She had much anxiety in respect to her pregnancy, especially when nurses told her of many cases of delivery unfortunate for both mother and child. However, the birth was quite regular. After childbirth the patient became fearful for the child who, she believed, could die at any moment. From the start she was a loving mother, forgetful of her own needs, and completely absorbed by her feelings for her child. From this and other observations, we see that she was ambivalent in her very egocentric and alterocentric changes of attitude.
Many difficulties arose due to bad relations between her husband and her mother. They were very different and disliked each other. Often there developed a feeling of two enemy camps between her parents and her own home. This situation troubled her very much. This unpleasant climate reached a critical stage when, following a family quarrel, the husband took his belongings and left to live with his parents. The patient then went through a nervous breakdown. She went through states of strong anxiety with strong psychosomatic reactions like being cold, going pale, etc. At times she went rigid or was in stupor.
When she was with her husband and child, or separately
18
with her parents, she felt very well. But when all were together, she felt very tired. Then her old fears returned. Once she went to bed with influenza after which her fears increased together with the feeling of estrangement. About this time, too, one of her friendly relatives died. From then on fears of death became prominent and the feeling of estrangement was intensified. This condition was somewhat improved after the use of Miltown (Meprobamate) and following a family vacation trip. She felt she was being cured. Soon after, however, she fell ill with nephritis, and fear symptoms reappeared. Her feelings of insecurity were increased by an atmosphere of resentment between the two family camps.
These reactions indicate that W.J. was much under the influence of her environment which pushed her towards positive or negative feelings. Since most of the time we do not observe in her autonomous dynamisms (consciousness, internal conflict) we can say that her developmental potential is limited in its expression.
With the coming birthday of her father, she attempted to influence her husband to come and wish him a happy birthday; her husband refused and this caused difficult moments for her. She had feelings of becoming insane. She did not sleep all night, and then had a nervous breakdown, similar to the previous one. She cried that she was dying; she felt her heart coming to a stop, and felt that she was losing consciousness. Electrocardiograph examinations showed no anomaly.
When her husband left for a few months to work out of town she felt a favourable decrease of tension in spite of all her true feelings for him. However, after a time her fears returned, especially her sense of estrangement and general weakness. An improvement in the family financial situation, the patient thought, would bring recovery of her health. But this was not the case.
At my request W.J. described her own character as that of a person universally sensitive with a sense of beauty for the world around her and possessing a certain fear before the forces of nature. She expected much attention from her parents and others to make her life easier. She spoke of herself
19
as having a tendency to be lazy, of being rather neglectful of her duties„ unsystematic, careless, and without internal discipline. She admitted a desire to be in the limelight, but without having to earn it; she lacked sufficient interest in the needs of others and looked at the world only from the viewpoint of her own self.
This opinion about herself indicates that she has the potential for an objective, negative, even sincere evaluation of herself. This points to certain potential in her to develop an attitude toward herself as object as well as to be capable of some initial process of inner psychic transformation.
A vivid imagination combined in her with a tendency towards an intense living of happy moments, looking for real fulfillment. However, she always lacked something which deprived her of reaching a full measure of satisfaction. According to her own account, she was not independent enough, since she needed to lean on someone emotionally, earlier on her mother, now on her husband. She said that some of her character traits were changed favourably under her husband’s influence; she became—in her words—more industrious and submissive, less hysterical (in the popular sense), and more attentive to her environment. On the other hand she thought that her husband could be a cause of her wavering confidence in her own resources, for he commonly told her how wrong she was. In her account she emphasized the divergence between dreams of happiness, wealth, great personal attractiveness, elegance, intelligence, and the reality which failed to fulfill those dreams. She thought that the change of atmosphere from that of a warm home environment to the challenging and difficult conditions of a mature life had increased her physical tension and fear of reality. This was connected in her mind with further fears of sickness and death.
The following conclusions about the presented material characterize some very important psychoneurotic traits.
1. W.J. is characterized by increased imagination and high emotional sensitivity. In this respect, every unpleasant experience provides a reaction out of proportion to the
20
stimuli; the degree of trauma caused by those stimuli is felt to be much greater than among so-called normal individuals. Because of that she showed an increased susceptibility to frustration.
2. W.J. grew up in a soft, even spoiling, climate at home. This together with her innate traits of sensual, emotional, imaginational overexcitability and egocentrism made her unprepared for the demands and responsibilities of marriage, which was for her too hard to adjust to.
3. Under conditions of great disharmony between the pressure of the external milieu and a poorly developed inner psychic milieu she lost the sense of proportion and balance in handling everyday affairs (weakening of the reality function). In consequence she developed fears. These fears or anxieties of indefinite character resulted in disintegration of her psychic unity. She was constantly worried “what is it going to be like,” she was worried about her appearance, she was afraid of an irregular pregnancy, she was afraid she would go, mad. These easily excited emotional tensions point to an enhanced excitability of imagination, affect and sensuality. Such enhanced excitability is the basis for a more intense perception of certain aspects of reality, hence for more anxiety. In consequence there is fear of these “other” aspects of reality and anxiety connected with the anticipation of that fear.
4. The patient possessed the capacity for easily transposing emotional experiences into the autonomic nervous system, manifested as spasms of the coronary vessels and disturbances of inner sensations (heart beating, nausea, head-aches, fainting, etc.). The attendant feeling of changes in personality structure manifested themselves in fears, especially of personality split and death. At times the patient reached a condition close to hysterical conversion with feelings of suffocation, trembling and stiffness of the body. Due to this manifest lack of inner psychic transformation the symptoms of conversion served as a
21
release mechanism for excessively strong stimuli and experiences. Their pressure, the lack of “damping” mechanisms, the lack of psychic organization made her defend herself by “rejection of response” (stiffness, immobilization, thoughts of death) as one possible solution, or by violent psychophysical responses (vomiting, accelerated heartbeat, headaches) as another possible solution. Her conversion tendencies, her fear before the coming of fear, were an expression of psychic panic in face of an insufficient capacity for inner psychic transformation, lack of a more serious preparation to carry “psychic loads.” The capacity to handle such loads appears only when there is a clear hierarchization and structuring of the “higher” and the “lower” in oneself. The “higher” is represented by the capacity for empathy, self-control, autonomy and authentism.
5. The patient exhibited a facility in changing from conditions of emotional upheaval, joy and enthusiasm to apathy and pessimism, accompanied by lack of thirst or hunger, headaches and feelings of insecurity. These symptoms can be correlated with her cycloid traits manifested in changeability of her moods: fears, depressions and insecurity alternating with excitement and enthusiasm. Excessive sensitivity, enthusiasm and joy had to be counter-balanced by sadness, depression, and pessimism. Such extreme expenditures of energy caused the opposite symptoms of psychic depletion, mental “shrinking,” energy shut-off, moving away (estrangement). Such reactions result from insufficient transformation of stimuli. W.J. did not have a higher center of control, or a center of hierarchization. Her life was evolving as if on one major plane only. Or one could say that she had only one level of polarization meaning that she was between two poles of her moods fluctuating between high and low, positive and negative, like excitement and depression
6. Excessive concentration on herself and living through unpleasant psychosomatic changes led her to the con-
22
viction that she was being observed all the time and that others saw these changes in her and that they regarded them as pathological. Because of that she had feelings of estrangement. Hence, worries about her features or complexion—fear to look into the mirror, fears of change, fears of being caught by surprise, fear of becoming insane, etc. She always thought she was in worse condition than she actually was. The weakness of hierarchization (inactivity of “higher” dynamisms) with great but one-level sensitivity towards herself and the environment precluded any reflection and change of the feeling of being observed by others. We see in W.J. a lack of a broader, more objective look at herself that normally leads to a broader, more objective and more conscious evaluation of oneself. She lacked perspective in looking at her own symptoms, was unable to interpret them to herself. Her mental activity tied as if to one plane lacked the sense of “multilevelness within oneself” which permits to take a look at oneself from above, i.e. from the position of higher processes such as self-awareness, self-control and others.
7. Signs of actual weakness, amplified by autosuggestion led her to a pathological need of always securing a free path of escape For example, in a cinema or theatre she occupied a seat near the exit; in an uncomfortable social situation she placed herself near the door. Increased excitability, introvertization and weak inner psychic transformation were the basis of a defense by way of “escape” or by way of releases involving little control.
8. The tendency to develop these conditions were innate (forms of her overexcitability, suggestibility, and nuclei of an ahierarchical inner psychic milieu were evident in her from childhood), and were intensified by the transition from a protective psychical atmosphere during childhood and adolescence on one hand, to less attractive environment during her adult life. The condition was aggravated by inappropriate upbringing (she was spoiled by her
23
parents) and her specific history of emotional experiences. Although she possessed these negative symptoms which were unpleasant to herself as well as to others, she was sensitive, individualistic, subtle, talented in some ways, and was very easily influenced in the development of her psychoneurotic condition. She was more susceptible to positive than to negative influences, but she was easily swayed by either. Thus we find a positive correlation between the symptoms of neurosis on one hand, and positive elements of the patient’s personality on the other. We see here distinct nuclei of positive development which had been arrested by lack of understanding on the part of the parents, her husband, and her physicians who treated her as ill and did not see her relatively rich developmental potential (emotional sensitivity, talents, highly altruistic behaviour when the members of her family were in danger).
9. Excessive sensitivity, excessive concentration on oneself, lack of a sufficiently rich syntony with the environment, lack of sufficiently developed hierarchy of values, a failure to develop a disposing and directing center at a high level all point to a lack of strong developmental potential.
10. She periodically expressed very strong interest in others, empathy, and readiness to help others in a deep way.
Nevertheless these relatively good nuclei of positive development did not find correspondingly good conditions in her environment, on the contrary, they were rather negative (she was treated as a hysteric).
In our view, several elements of her personality did not permit a sufficient, positive mobilization of her rich developmental potential, although weak in autonomous factors. Among these we would include her hypersensitivity, a great facility for transposition of psychic experiences into the autonomic nervous system, her lack of development of psychic independence, and a disproportion between excessive sensitivity and in-
24
sufficiently strong sense of self-awareness and self-control. Furthermore, there was a lack of external stimuli which could help promote a certain degree of emotional resilience—all these elements did not permit a sufficient, positive mobilization of her rich but unutilized developmental potential.
From the standpoint of the theory of positive disintegration the stimuli she received were insufficient to mobilize and develop an inner psychic milieu, a hierarchy of aims, a disposing and directing center at a high level, or any interests and talents as well as autopsychotherapeutic dynamisms.
In conclusion let us compare the negative and the positive elements of W. J.’s development:

25

Case 2
S. Mz. was 34 years old. She had a Master’s degree in engineering. She came with complaints of sleeplessness, depression, feelings of estrangement from herself, and a tendency to self-mutilation. She has suffered from these for many years. There were numerous symptoms such as weakening of powers of atten
26
tion and concentration, disturbances in mental work, and weakening of memory. Furthermore, she experienced a rather definite decrease in will power; she could not force herself to work.
The patient was treated with several varieties of tranquillizing drugs. She went through two out-patient insulin therapies. Her condition then improved, but only to deteriorate soon after. An especially important aspect was a depression accompanied by a tendency for escape into the world of fiction. The patient, as she herself said, was in a catastrophic personal situation. However, she did not care for an acceptable standard of living. Every deterioration of her living conditions brought her to a state of “psychic harmonization.” At the same time her reaction, to any stupid or fiat remark was very strong, almost physical. She was always far from the realities of life, living “in clouds.” She stated that she had no “emotional temperature”; she could not love or hate anyone. She liked to create theories of social, moral or philosophical nature.
Her life was difficult since her mother had brain sclerosis. She was professionally capable, but her working conditions became difficult; she was often treated maliciously. She was strongly emotionally attached to a man who died of a serious, incurable disease. This was a destructive experience for her. More recently she could not sleep at all, except after taking Evipan (Hexobarbital). She had feelings of estrangement from herself and thought she was becoming schizophrenic. Yet this was to her a consoling thought. She would have liked to be in a hopeless state. She came hoping to hear confirmation of her pathological condition.
She did not have any negative developmental potential (i.e. no evidence of psychopathy, mental retardation or psychosis); her positive potential was manifested early as an emotional and imaginational overexcitability combined with a predominance of introvertive traits.
General medical and neurological examination:
Thin, somewhat weak constitution, strong trembling of eyelids, slight trembling of hands, light pulse, low blood pressure, ex-
27
cessive and strongly inhibited muscular reflexes, increased and extended red dermographia.
Strong trembling of eyelids, moderate trembling of hands and enhanced muscular reflexes indicate (in the absence of organic changes) an increased psychic overexcitability and also certain degree of disharmony between excitation and inhibition. Such interpretation denotes an introvert type with a tendency to excessive inhibition.
Descriptive diagnosis
Asthenic, schizothymic, introvert, with exceptionally high emotional sensitivity and imagination, weak tension of reality function (i.e. in regard to her external affairs and her work) at a low level, tendency to dwell on things transcendental. Inadequate adaptation to reality, low vitality. The dominating difficult experiences with which her personality could not cope resulted in fatigue and emotional exhaustion, in feelings of emptiness and estrangement from reality and from herself as a real being. Injustice, disappointments, suffering and exhaustion resulted—as is the case with many individuals of this type—in an attitude of “completing the defeat brought by fate and bad luck” through self-mutilation, and an apparent need for experiencing the worst, even death. The disposing and directing center was represented by the tendency towards self-destruction and self-annihilation. We observe here a reversal of the usual hierarchy of values and goals. The supreme “value” and `goal” here becomes death itself; the death instinct takes on the role of the disposing and directing center.
Clinical diagnosis
Psychasthenia with a strong component of depression; possibly a borderline case of schizophrenia.
Justification of diagnosis from the standpoint of the theory of positive disintegration
S. Mz. shows disorder of functions and psychosomatic suffering resulting partly from constitutional characteristics (emot-
28
ional and imaginative overexcitability) which are aggravated by strong and difficult experiences. At the same time we notice a high level of mental sensitivity, a distinct development of moral feelings, and a tendency towards cultivation of exclusive forms of emotional attachment. This last tendency is a natural consequence of her enhanced emotional excitability which is one of the components of her developmental potential. She showed this emotional overexcitability rather early in life. As a child she was stubborn, emotionally independent and in a childish way independent in her thinking. At times she also suffered from anxieties. However, the unfavourable conditions of her life prevented the development of all her psychic resources.
A characteristic feature is the differentiation of reality function into two levels. The lower level (coping with external affairs, her job and everyday living) underwent almost complete atrophy whereas the growth of the higher level was unequal and in part excessive. It was represented by her moral sensitivity and search for philosophical answers to the meaning of her life. Weakening of the instinct of self-preservation was accompanied by the appearance and intensification of the instinct of death and tendency toward self-destruction.
This patient represents a clear instance of multilevel disintegration, even if limited in scope. We are dealing in this case with such strong forms of emotional and imaginational overexcitability and with such distinct introversion that under the impact of grave experiences and also the pressure of complex experiential contents, there appears to take place a not totally conscious uncovering of the basic dynamisms of positive breakdown. There is high tension, frantic search for solutions, realizations of the instinct of partial death, striving for the atrophy of lower level functions, seeking suffering) with an ambivalent mobilization of suicidal tendencies, supersensitive hierarchization of values, transposition of the reality function to a higher level (i.e. into the world of fantasy, imagination and transcendental problems).
The therapy should concentrate upon developmental and creative forces both in the patient’s inner psychic milieu and
29
in her external environment. These forces should be used to increase her interest in life and to promote further mental growth. Despite her depressions and suicidal tendencies she had a high level of enthusiasm which could be awakened by strong authentic agents (e.g. getting involved in valid and important philosophical or social movement, great love or friendship). Such development has to take into account further intensification of creativity; it needs to include a search for existential under-standing, a search for new friendships to be developed with a deeply empathic attitude. It would be absolutely necessary to help her find such friends.
Case 3
S.P. was a priest 26 years old. He came seeking advice regarding feelings of insecurity, scruples and an inability to see what is a sin and what is not. The patient was sensitive and nervous from childhood; he was attracted to the life of prayer, and to understanding and helping others. He entered the seminary since he felt it was his vocation to help others as a priest. For several years he had recurring doubts as to whether he thought and acted properly. He had feelings of inferiority, and was convinced of being worse than others. He did not remember well positive things about himself and his actions except those that had a “shade of sin.” The feeling of his sinfulness often grew out of proportion. If he saw a poor or sick person or was a witness to violence and could not help, he had feelings of guilt and of having failed in his duty. He was very sensitive to the feelings in people and animals. The possibility of causing sorrow to another person made him feel very uneasy. He was in perpetual doubt whether his confessions were good; he kept wondering if he did not omit something. He thought God will judge him severely. He feared professors and examinations. There were no sexual problems.
General medical and neurological examination:
Ascetic look, concentrated face, deep-set eyes, gentle and humble attitude. Pulse rate normal; trembling of eyelids; blood
30
pressure 150/80; red dermographia pronounced and prolonged. High ability to transpose psychical experiences onto the autonomic nervous system exemplified by irregularity of his pulse under emotional stress, sweating, red dermographia, blushing.
Descriptive diagnosis
Individual with a high degree of sensitivity since childhood. He was educated in a cultured milieu in a family with strict moral demands. A contact introvert type (Rorschach). He was meditative, inclined to exaltation, and was striving for the formation of a disposing and directing center at a higher level, tending towards the personality ideal. He was shy and hyper-sensitive, susceptible to moral scruples and states of existential anxiety. His life-experiences developed into a process of multilevel disintegration, with its characteristic dynamisms such as feelings of inferiority, dissatisfaction with himself, feelings of guilt and sinfulness.
Clinical diagnosis
Obsessive psychoneurosis.
Justification of diagnosis from the standpoint of the theory of positive disintegration:
His excessive sensitivity, scruples and fear, excessive feelings of inferiority and sinfulness arose from his innate increased sensitivity and his educational background. His enhanced emotional and imaginational excitability was combined from childhood with nuclei of the potential of a hierarchy of values (authentic vocation, early developed inclination for prayer and meditation, early developed sense of guilt). Justification of others and severity in regard to himself express the development of empathy, humility, readiness to be “against himself” which is a form of isolating in himself the subject and the object. All this is an expression of strong tendencies to differentiate within oneself higher and lower values, that “which is” and that “which ought to be.” There is a clear formation of the instinct of self-perfection.
31
Therapy:
What he needs is to spend less time alone and more in everyday pastoral involvement. At the same time attempts should be encouraged aiming at self-conscious overcoming of anxiety and excessive scruples.
The patient should be able to understand and to accept that his development is “normal” and healthy within his type, and that his scruples and feelings of guilt need to be brought into his whole program of personality development as positive elements. Nevertheless it would be necessary for him to diminish their tension by stressing more the development of social involvement, contact with nature, in order to re-channel his attention which was centered too much on his failings.
Case 4
J.S. was 21 years old. She sought psychiatric help because of her anxieties and obsessions. She was rather nervous since childhood. She exhibited fears of space, of riding autos and street-cars; she was afraid to go out on the street by herself. At night she frequently woke up with feelings of anxiety, cried and could not fall back to sleep for a long time. She developed various obsessions, as for example when she kept thinking of the number 8. She could not get rid of it and this recurred in a very unpleasant way. When shopping and intending to buy a certain number of products, she kept thinking of different numbers besides those related to the shopping list. When entering a store or a friend’s home, she always went in sideways since she was afraid that someone would attack her. Several years ago she witnessed a fatal accident; the streetcar in which she was riding ran into a man and killed him. This increased her fear of auto or streetcar riding. At another time, her father when drunk threatened to kill himself with a razor. She then developed an anxiety condition. She was married and had a sexual life with no disturbances.
General medical and neurological examination
Eye pupils very large; strong trembling (of small amplitude) of eyelids and hands; pulse rate somewhat irregular; blood
32
pressure 120/80 (variable). Oculocardiac reflex positive, with tendency to arrhythmia.
Strong trembling of hands and eyelids, wide pupils, irregular pulse and oculocardiac reflex tending toward arrythmia point to increased psychic excitability and facility for switching emotional experiences over to the nervous system rather than resolving them consciously.
Descriptive diagnosis
Since childhood she displayed excessive psychical sensitivity. She suffered from anxieties and sometimes would be in a “psychic panic.” She cried often and easily and even in a childish way she was not capable to understand what really was happening. Her repressed dynamisms acted through the subconscious, because she avoided thinking about her grave—even tragic—experiences. This attempt to forget did not work and these experiences would return suddenly and without warning when she was feeling good and having a good time. Sudden unexpected events, even if not very threatening, caused in her traumatic reactions. She lived in a state of dramatic suspense before some undefined tragic event, most likely as a result of the incident when her father tried to cut himself with a razor. In consequence she had the need to secure avenues of escape in case of an unexpected danger. This would also account for her occasional panic.
She was asthenic and schizothymic. This denotes tendencies to move away, to be asocial, to have strong imagination, and even tendencies for loosening and disintegration of the personality structure.
She had distinct deficiencies in inner psychic transformation. In her case these deficiencies took the form of a fear of space which was not easy to change. Also in other areas she did not show signs of a distinct developmental potential. The traumas of her childhood blocked her limited abilities for development of spontaneous multilevel disintegration. She was oversaturated with traumas and shocks, her consciousness was narrowed to a limited range of phenomena and stimuli.
33
Clinical diagnosis
Anxiety and obsessive psychoneurosis with considerable reactive elements and somatic components.
Justification of diagnosis:
Functional sickness. Excessive psychical sensitivity. Reactive neurotic elements. Facility of transposing emotional experiences onto the autonomic nervous system as shown by her neurological examination. When she was examined (a medical examination almost always induces some psychic tensions in the examined) she reacted with a positive oculocardiac reflex, sweating, irregularity of pulse, etc.
One can observe in this case the greater controlling power of harmful external elements, of the influences of her social milieu than her developmental potential which is rather weak. She does not show a controlled conscious attitude in respect to her own symptoms. One does not observe in her any clear ability for transformation of her psychoneurotic experiences and their utilization in order to distinction of “higher” and “lower” elements in her mental structure.
Therapy
Quiet, easy life, pleasant experiences of a wide scope, widening of interests, sport, gradual formation of conditions favorable to the transition from unilevel to multilevel disintegration. If a person has a certain degree of emotional and imaginational sensitivity and suggestibility then one can attempt to effect this transition by trying to exert more influence than the patient’s environment has in the following way. One can suggest to the patient a more conscious approach to herself and her social milieu by stressing her positive qualities (her sensitivity in particular). One can at the same time suggest to develop certain insensitivity and independence from the influence and suggestions of her social milieu. An orderly and quiet life as mentioned above is here advisable.
There should also be created conditions of feeling secure and of increasing feeling of responsibility towards her family.
34
It would also be of some value to ask the patient to repeat the following sentence: “What is the worst that can happen to me?” in order for her to develop an ability to face and handle unpleasant events in her life.
A gradual introduction of stimuli and experiences somewhat difficult and unpleasant but of not too high tensions would also help the patient to control little by little minor difficulties and changes.
The behaviour therapy techniques which, by the way, were not yet developed at the time this patient was treated, would appear to be the most practical means of handling her phobias (Wolpe, 1958).
It would also be meaningful for the patient to develop her sense of humor both in relation to herself and to others.
Case 5
This case is taken from Pierre Janet (Murphy, 1929) and concerns a twenty-year-old girl Irene. Unfortunately Janet does not give the exact life history of the patient, her interests and characteristic emotional attitudes in her normal period.
Irene became sick in despair over her mother’s death at which she was present. This happened under dramatic conditions in a small workman’s room. She was overcome with strong nausea, blood-vomiting and several other strong symptoms. The young girl was fighting with the thought of her mother’s death. She brought herself to total exhaustion since the last sixty days before her mother’s death she did not go to bed. Instead, she periodically left her dying mother and went to work in order to earn her living. After her mother died, Irene wanted to resuscitate her body and bring back respiration.
Sometime after the funeral, Irene exhibited strange symptoms. She developed somnambulism and played dramatic scenes of great artistic perfection. She brought to life in all detail and with skill, all the drama she had recently lived through. She was narrating the content of these tragic scenes, putting forth dramatic questions and answers (tragic dialogue), listening to her own questions, introducing a tragic spectator to the drama,
35
she took up a variety of postures according to her role. She combined words with gestures and actions which gave an unforgettable effect. When the show was about to end she made ready to die. Then she talked with her mother and made the decision to die under a moving train. She put herself on an imaginary railway, waiting impatiently for a train to came and with horror in her expression and posture, showed deep experiencing of reality. The train came, she then got up and some scenes of the sequence were reproduced again identically. After a time she became exhausted, and returned spontaneously to her former state of consciousness and continued her ordinary daily tasks.
Descriptive diagnosis
We observe here first of all exceptional concentration of feelings towards her mother together with a weakening of the instinct of self-preservation. Irene appears to have strong vitality (care for the home), with a capacity for sacrifice and almost heroic acts in the performance of her duties, which were carried out with exceptional fidelity. She was under such great pressure and exhaustion that there followed a psychical split, a disintegration. This state of tension finds its outlet in two life patterns: one is ordinary reality, the other—the content of dreams.
We know nothing of the patient’s intellectual standing. Still, her capacity for expressing what she experienced excludes mental retardation. Besides, we know from the description of the case that Irene was making her living, that she knew how to administer artificial respiration, etc.
It appears that she had not adequate transformational abilities. Due to this limitation, high psychical tension led to a split into two personalities as it were, which—it seems to me—was a safety valve against suicide or developing schizophrenia. As we have pointed out, her emotional tension, empathy, and many capacities were of the highest level, but the dynamism of inner transformation was rather weak.
36
Justification of diagnosis from the standpoint of the theory of positive disintegration:
The symptoms are characteristic of unilevel disintegration with the exception of the moral sphere. The patient shows distinct excitability of the emotional and imaginational type, the need for strong and lasting emotional bonds, great moral sensitivity and a distinct hierarchy of moral values that indicate the beginning of multilevel disintegration.
Therapeutic recommendations
Irene needs cordial and warm human climate and assistance in working out a program of further education and sublimation of her emotional life. The development of artistic abilities (acting and drama) may help her to find the sense of life. It would be strongly indicated to introduce her into a circle of friendly and understanding people.
Comparative Analysis of the Five Cases: Unilevel vs. Multilevel Disintegration
All the cases presented above are characterized by an enhanced excitability of emotions and of imagination, in case l, also of sensuality. In all cases, except case 4, it can be considered as indicating positive developmental potential. In all cases, except 4, there are nuclei of the ability to see and to experience levels of reality other than the level of everyday life. This is particularly evident in cases 2 and 3, but much less in case 1. All cases are marked by more introversion than extraversion. In consequence of such typology the individuals cannot look for solutions of their difficulties in the external world but mainly in their inner world. The way open to them is a development through painstaking uncovering of higher dynamisms in themselves (e.g. personality ideal, empathy, self-awareness, a sense and philosophy of life). Case 1 and 5 show weaker tendencies in this direction, while case 4 shows none.
Case 1 is characterized by “escape” into conversion, sickness, split personality, the territory of the unconscious. Cases 2 and
37
3 are not satisfied with such solutions. They are bound to look for hierarchical solutions in the evolution of higher and higher values and in the dwindling of the lower ones.
In case 1, where there is lack of a distinct hierarchy of values but there is a great general psychic sensitivity and creative abilities, this “hierarchy” in combination with an altruistic attitude appears under conditions of danger to close persons. The mobilization of this “hierarchy” is possible only when there are very strong stimuli.
In case 2 there are such strong existential tensions with a history of such intense suffering that there is danger of the total loss of the sense of existence. As a result there is a break-down of psychic structure and of relating to external reality. There are three possible solutions to such a situation: suicide, mental illness, or very sharp emergence of a new hierarchy of values.
Case 3 presents tension of sensitivity and of introvertization leading—through scruples and feelings of guilt and sin—to developmental projection bordering on mystical life. Here the patient’s task is to partially “step back” from himself and come to the realization of empathy in social action.
Case 4 appears not to have any developmental direction. It is tied to one level and its perturbations and tensions. It is under the influence of unilevel unconscious contents.
Case 5 presents a somnambulic split of personality caused by an impossible to bear tension and by an insufficient ability for inner psychic transformation to reach higher levels of a hierarchy of values. In view of the developmental deficiencies the split of personality is a method of handling the experienced tension and defending oneself against such dangers as psychosis or suicide.
In cases 2 and 3 the developmental potential is stronger than in cases 1, 4 and 5. The same is true for inner psychic transformation, special abilities and talents.
When we further compare these cases we see that cases 2 and 3 represent several levels of emotions and of values and
38
consequently have conflicts between these levels. In cases 1 and 4 the experiential processes proceed as if on one plane only. In cases 1 and 5 higher levels of emotions are activated under the impact of very strong emotional stimuli. Thus we can say that these three cases are examples of unilevel disintegration (case 1 is actually on the borderline of unilevel and multilevel disintegration) while cases 2 and 3 are examples of multilevel disintegration. We call it multilevel because there is an observable hierarchy of mental functions. Very often the higher levels are the controlling ones with ensuing tension and conflict with the lower levels. Such conflicts are conflicts of choice (conscious or unconscious) in which the person feels what is more desirable but is unable to follow it without opposition of the less desirable but still present and active (and at times controlling) lower levels. In this sense these are conflicts of value. Conflicts of value entail the existence of feelings corresponding to higher and lower values. We thus have a hierarchy of values, or of higher and lower levels of emotions. The process of developing or activating these different emotional levels is called hierarchization. The table below puts together the types of disintegration and the process of hierarchization for the five cases.
TABLE I
Disintegration Hierarchization
Case 1 Unilevel Rarely active
Case 2 Multilevel Active but not always conscious
Case 3 Multilevel Active and conscious
Case 4 Unilevel None
Case 5 Unilevel Active but not conscious
39
CHAPTER III
NEUROSES AND PSYCHONEUROSES
1. Neuroses and Psychoneuroses as Disorders of Functions
Psychoneurotic symptoms and psychoneurotic dynamisms are strictly related to emotional perturbations. These perturbations can be either positive or negative. They involve all levels of the brain, and especially the frontal cortex. Neurophysiological and neuropsychological investigations have localized in the frontal cortex the highest autonomic functions together with the highest centres of emotional life. There is a strict relationship between emotional functions and the functions of the autonomic nervous system. So-called psychoneurotic disorders are, therefore, emotional perturbations occurring on different levels of the nervous system. Almost always they involve the excitation or inhibition of frontal centers.
The terms “neurosis” and “psychoneurosis” thus far have not been clearly defined. We shall apply the term “neurosis” or “somatic neurosis” only in those cases where physiological components (organs or systems of organs) are involved. Neuroses in their pure form are psychosomatic or psychophysiological disorders. The functional components involved do not show any organic changes. The disorder is thus not a defect of structure but of function only.
Psychoneurosis is a disorder of function, which like neurosis, is reversible, i.e. it can be “cured” or even transformed into a developmentally higher form of psychological functioning. This higher form is no longer a psychoneurosis but a new personality structure in which the psychoneurotic history remains recorded. In consequence there is a special sensitivity for others (depend-
40
ing on the particular history of the ex-psychoneurotic) who suffer from obsession, depressions, anxieties, fears or show hysterical reactions.
Psychoneurosis in comparison with neurosis represents a “hierarchy of higher functions,” which means a hierarchy in which mental dynamisms predominate over nervous reactions. Psychoneurosis is a more psychical or more mental form of functional disorder, while neurosis is a more nervous or somato-psychic form.
Neurotic disorders concerning inner organs (heart, stomach, genitals) are called neuroses of organs. Neurotic disorders concerning a wider system of organs and functions (circulatory, digestive, urogenital systems, etc.) may be called neuroses of systems. There are also so-called “migratory” neuroses, i.e. those which move from one to another organ or system. This “migration” depends essentially on two factors: one, an excessive strain on an organ or system of organs involved, and two, the degree of tension that can be handled by a given organ. By transfer to other organs “migration” helps often to equilibrate strain and tension.
Neuroses can be expressive of hyperfunctions, hypofunctions or dysfunctions; they may be of a briefer or longer duration; they may localize in a specific system, or extend to several systems. However, hyperfunction in one organ or in a part of a system can coexist for a brief or longer period with hypo-function in another organ or system. These conditions can also vary since there is a tendency to change the localization of excessive tension.
Neurotic symptoms may be effects of psychical difficulties and disorders, or, such symptoms may be partial or additional causes of those disorders. Psychical trouble may attack the weakest points of inner organs; it may be “localized” in them. Neurotic disorders may be expressed in abnormal functioning of fundamental biological processes as a consequence of an inadequate diet (overeating or unbalanced diets), sexual habits which are selective and often rare, like excessive tendency to sexual associations with visual or tactile stimuli (also fetishism,
41
necrophilia), or any other, which is shown in both malfunctioning of the respective organs and simultaneously, or subsequently, in mental disorders.
A poorly functioning organ or system of organs brings about both organic and mental consequences; on the other hand, abnormal or supernormal emotional or mental experiences such as fear or anger, depression or one-sided ecstasy, may cause vascular, muscular and other disturbances. With an existing neurotic background, strong emotional stimuli which disturb the normal action of consciousness may further complicate neurotic disorders (for example, bring about a tendency towards flight into sickness), or they may compensate them. They may then be expressed by more or less acute symptoms such as spasms of the stomach, asthmatic attacks, menstrual disturbances or speech difficulties. These result from an inability to resolve emotional tensions and conflicts on the psychical level alone. The psychical level is not prepared to handle them; therefore, experienced difficulties are transferred to that level of the autonomic nervous system which controls the function of the body as an available territory for localizing internal tensions. On a higher level of emotional development the difficulties are handled and transformed at “higher psychical levels.”
Specific individual relations exist between particular systems of somatic functions and psychic structures of the individual. This relation may be a germinal form of conflict between somatic tendencies of various levels of the nervous system and the many levels of psychical functions, conscious or unconscious, formed through educational habits or organized through process of education of oneself.
The degree to which the psychical element will influence the somatic one depends on the level of general development, the manner of development of the disturbance, on the degree of consciousness of the suffering individual and on the possibilities of conscious or subconscious influence on the progress of the disturbance.
Pavlov, for example, spoke only of neuroses. His basic assumption was that the organism exists only as physiological whole;
42
some of its physiological functions are related to cortical functions, and are called psychical phenomena. This view is not uncommon even today. Detailed studies indicate, however, that in every case of neurosis, the human psyche is involved, and in, a large majority of cases (if not all) of the type described (e.g. cases 1 through 5, Chapter 2), there is a more or less strong neurological disturbance of organs or systems of organs as well. Psychosomatic hypersensitivity or psychosomatic “allergies” are, different terms to describe the same phenomenon.
2. The Disturbed Function
Pierre Janet, recognized neuroses as a disturbance, or an arrest in development, of a psychical function, but without damage to the function.
It is possible to have a function disturbed or arrested in its development for long, without resulting damage? This indeed is possible; however, let us keep in mind that our discussion concerns complex emotional functions in the adult which develop after the brain has been fully formed. For instance in cases of hysterical paralysis it may happen that the individual is “cured” and is able to move his previously paralyzed limbs, without any difficulty and without any retraining, he can run, dance, take up sports, and so on. Similarly in mutism which can last months or even years the “sick” person may return abruptly to the full use of speech.
Some forms of catatonic schizophrenia, like “flexibilitas cerea” (waxy flexibility), with mutism, complete inactivity, autism, and strong somatic disorders, permit at times a return—after several years, or even some decades—to complete psychophysical fitness.
3. “Arrest” of Development
While the condition of “functional disorder” would not cause great concern, the condition of “arrest in development” is a cause of such concern. Withdrawal is often considered an arrest in development. For instance periods of isolation from the social environment, which for some psychasthenics may last a long time, do not affect adversely their deeper relations with
43
others in the sphere of inner experiences, imagination and creativity. Also, one can get away from difficult and fatiguing situations at work, from stresses of a given milieu in order to seek the refreshing change of a different and carefree atmosphere. Childish games, contact with nature or art, friendship and love, all serve as refuges of rest and sources of new energy. This change of field of action to simpler activities and relationships heals “psychical wounds” and prepares for new difficulties. Such prophylactic withdrawal which builds greater resistance can be called positive regression.
An arrest in the functioning of a certain system may indicate stoppage of the functions of that system, but not necessarily of global development. A temporary arrest or stoppage of some function as a result of fatigue often helps in its further development following the period of rest. For example, emotional exhaustion may arrest current interests, contacts and activities and call for more sleep, isolation, daydreamings, in short, may lead to a form of “regression.” Eventually such “regression” may enhance and deepen individual growth. This happens in the case when the period of “regression” introduces new and higher dynamisms that previously could not develop because the established mental and social activity of the individual did not allow them any room.
Some traits related to certain developmental types (e.g. psychical infantilism), temporarily out of sequence may also undergo reversal with compensatory accelerated development. We believe that such disturbances as hesitating tendencies, psychical disequilibrium, increased psychical sensitivity, and temporary weakening of some function or system of functions often provide considerable possibilities for personality development. These hesitations, states of disequilibrium, enhanced excitability, shyness, etc., are stimuli for reflection, for developing a more subtle attitude towards oneself and towards others, for experiencing and absorbing new contents which if acted upon too quickly would result in a limitation, or even loss, of the possibility of expanding emotional experiences and their understanding. I quote one of my patients: “It is only now that I begin to see what a blessing to others are some of our inhibitions and hesitations;
44
how much harm we do when we act impulsively, when we are, too sure of ourselves, when our decisions are made easily without taking others into consideration.”
4. Neuroses and Psychoneuroses: Commonness of Occurrence
The incidence of neurosis and psychoneurosis is largely dependent on cultural and technological changes in society.. According to Brun (1954) about 70 percent of all the patients of Swiss public dispensaries are neurotic patients. In France about 80 percent of all absences from work due to sickness are attributable to neuroses. It is not much different in the United States (Srole et al., 1962; Leighton, 1956).
In Poland, on the basis of fragmentary data from some state hospitals, the number of neurotic patients rose to 30-40 percent of all patients in the department of internal medicine, where patients with neurosis are being admitted. It should be understood that those are the more serious cases of neuroses, and therefore less common among the total number of neurotic sufferers. Those who come for out-patient or sanatorium treatment are but a small fraction of all psychoneurotics.
A majority of the sick do not consult the physician. They are those who are aware enough of the whole complication, of their disturbances; they realize that the cure would necessitate several months, perhaps years of great effort, and require exceptional knowledge combining neurology, psychiatry and psychology together with a high moral authority on the part of the therapist; all those values can rarely be provided by the ordinary physician. Those patients treat themselves, through autopsychotherapy, and rarely use advice and pharmacological prescriptions for less essential, “marginal” components of their suffering. A great majority of nervous children and adolescents—those who developed a neuropathic component—have: a high level of ability. This is another complicating element which provides a basis for the development of “educated awareness” often this is the basis for a feeling of superiority and resentment. towards physicians who possess inadequate comprehension or a careless attitude with regard to their patients' suffering.
45
A second group of psychoneurotics is composed of those who do come for therapy. They are people whose capacity for adjustment to life has been considerably diminished and whose independence with respect to the environment and the capacity for autopsychotherapy are much limited. Hence a great majority of cases present a picture much different from that described previously. Among those treated as ill there appears much helplessness, passivity, low level of performance at work, and low level of consciousness plus some negative, infantile forms of behavior.
Within the first group—by far the more numerous—we find that almost all the individuals can, with a lesser or greater degree of effort, take care of themselves, their problems, and those related to their environment; on the other hand, the much smaller second group usually cannot deal with themselves and with their environment.
According to my observations, to the first group usually belong intelligent not infrequently outstanding, individuals, having psychical structures capable of high, even accelerated development through positive disintegration (Dąbrowski, 1967; Dąbrowski, Kawczak, and Piechowski (1970). Those belonging to the second group are, in the majority of cases, inclined to psychical bankruptcy, possessing largely involutionary structures, and are inclined toward tendencies which arrest their personal development. They usually exhibit little creativity in the disintegrative process. They have a limited developmental potential (see Chapter 1).
5. Classification of Psychoneuroses
Considering the present state of knowledge, the problem of classification of neuroses and psychoneuroses (Dąbrowski, 1963) is, in our view, of secondary importance. We take it up, however, in order to more fully acquaint the reader with our point of view. First of all, the general basic condition for the genesis and development of neuroses and psychoneuroses is—in our opinion—an increased psychical excitability. This is expressed in increased excitability with respect to emotional, psychomotor,
46
imagination, sensual and intellectual areas. Increased psychical excitability, expressed in so many ways, is the constitutional background of neuroses and psychoneuroses which exhibit somatic components; they modify psychical syndromes and are in turn modified by the latter. This subject is further developed in Chapters 6 and 7.
Among psychoneuroses we can generally distinguish the following
1. Psychasthenia; expressed as a general psychical weakness, lowered tension in basic drives, disturbances in reality function, reduction of social contact, at times with obsessional components.
2. Psychoneurotic obsession; characterized by pathological perseverations, scruples, tendency for fixation to certain things, thoughts, feelings, defined forms of action. Here also belong, but rather marginally, tics as a resultant of enhanced psychomotor excitability and obsessional tendencies.
3. Psychoneurotic anxiety; acute, sub-acute, or chronic symptoms such as fear, anxiety, timidity, and specific forms of anxiety such as night anxieties, anxiety before interrogation, phobias, etc.
4. Psychoneurotic depression; decrease in psychical functions, excessive tendency for self-analysis, self-criticism, feelings of inferiority, guilt, etc.
5. Psychoneurotic infantilism; expressive of conditions of excessive excitability, wavering in psychical attitudes, sadness, negativism, and other infantile characteristics, including tendency for animism, artificiality, magical thinking, “psychical immaturity,” tendency towards emotional immaturity and regression, etc.
6. Hysteria; excessive emotional excitability and suggestibility; disturbances of the reality function, tendency for conversion of psychical into somatic disorders and vice versa, changing goals or behavioral patterns, instabi-
47
lity, suggestibility, lack of moderation, breakdowns of an exhibitionistic character.
7. Sexual psychoneurosis with disorders such as hypersensitivity towards sexual stimuli, sexual inhibitions and timidity, premature ejaculation, strong tendencies toward masturbation, borderline symptoms of psychoneurosis and perversions.
With respect to organ neuroses and neuroses of systems of organs, we apply the following classification:
1. Digestive system: a) acute colitis; b) chronic mucomembranic inflammation of the colon; c) spasm of the pylorus (pylorospasm); d) fecal soiling (encopresis or involuntary excrement rendering); e) nervous lack of appetite (anorexia nervosa).
2. Respiratory system: a) general disorders of respiration; b) allergic bronchial asthma.
3. Circulatory system: a) acceleration, slowing down or unevenness of pulse; arrhythmia; b) migraine.
4. Urogenital system: a) intermittent urine-rendering (so-called “stuttering” urine-rendering).
5. Miscellaneous sexual neuroses.
6. Muscular system: hyperkineses, tics, etc.
In reality we rarely encounter neuroses of distinct organs. When diagnosed, they usually prove to be only dominants among the numerous neurotic disorders of other organs or even of other systems. For example, heart neuroses are usually related to functional disorders of the vascular system. With spastic neurosis of the colon we often find spastic symptoms in other areas such as the vascular or urogenital systems. The so-called “migratory” neuroses are known to move from one system to the next. The same is true of psychoneuroses, e.g. obsessions are often associated with psychoneurotic anxiety or with psychasthenia, with a varying dominance of this or that syndrome.
48
CHAPTER IV
PSYCHOSOMATIC CORRELATIONS
1. The Role of Subcortical and Cortical Centres
The development of a young animal differs from that of the newborn human in that motor functions in the animal are under the control of sub-cortical centers whereas in the infant, they are under the control of the cortex itself. The participation of the cerebral cortex may be the cause of a longer period of elementary development of the human infant.
At the end of the first month of life, the cerebral cortex is already operational in an infant; this is shown by his ability to form conditioned reflexes in all sensory modalities. However, the baby’s movements in this period are uncoordinated. More complicated movements such as crawling, sitting up, walking and talking develop much later. The flexibility of the central nervous system, the lability of its centers and of their particular physiological elements, increase with the development of the organism.
Psychoneurotic individuals are characterized by high lability of the nervous system. The apparent lack of motor skill is manifested among psychoneurotics by uncertainty of movements, by a tendency to leave things unfinished, and by shyness or timidity—restraint, fearfulness, timidity express themselves in constraint of movement, in hesitation and changes of mind, difficulties in making a decision, which indirectly affects the flow of movement and often gives impression of ineptness.
These symptoms are related to “stuttering” of somatic functions, conflicts with oneself and with the environment, cyclicity of moods, and “autonomic disorganization.” Lack of motor skill is often associated with being impractical, with a weakening
49
of the more primitive psychical structures—the integration at lower levels is thus partly lost.
The subcortex integrates instinctive and emotional functions on a lower level. This integration of basic functions is guided by avoidance of pain and search for pleasurable satisfaction. Animals are guided principally by subcortical enters and it is characteristic for them to acquire in a short period after birth their sensory and psychomotor proficiency.
The integrating ability—the globality of functional performance which is directed by sub-cortical centers—diminishes as the functional loci of control move up to the cortex.
The functions of the cortex are much more complex. It is an organ of association covering a wide range of inputs, including higher emotions and higher drives. The cortex is an organ of control. In my opinion the frontal cortex is not only the organ of conscious control but the organ of conscious personality growth coupled with higher instincts and intelligence.
The development in the direction of cortical functions—and ultimately of frontal functions—does not occur quickly or smoothly. The inhibition and control (or even extinction), as well as the transformation, of lower ones does not occur uniformly and globally. Hence the disintegrative-integrative activity of developing cortical functions is uneven in its effect on the sub-cortical functions. In consequence the neurotic, and especially the psychoneurotic, processes gain in intensity.
This is associated with inhibiting actions with respect to lower functions, and excitation; or increased sensitivity with respect to higher functions (inspiration, creativity, ability for prospection).
2. Release of Tension
We observe in psychoneurotic the development of hierarchically higher nervous processes (e.g. reflection, meditation), rather than practical everyday skills, or psychomotor skills, and a tendency towards excessive inhibition of lower level functions This is characteristic of the majority of psychoneuroses. In certain cases of psychoneurotic disinhibition and “explosivity,” there is
50
a manifestation of the tendency to return to more integrated positions, to submit to the more primitive directions of well-organized sub-cortical centers, back to a well known, and secure level. This takes place when the individual cannot achieve a higher level of equilibrium while the experienced tension exceeds his limit. Dostoevsky said that when he experienced the sublime and the ideal, just then as if through a psychical fissure leaked in “basic” impulses (sexual, aggressive, and the like).
Hysterical tics or nervous crises also indicate the descent to the level of the sub-cortex. Their persistence and the difficulty of eliminating them shows that they are partially integrated and narrow, as though parts torn from the whole, which then became autonomous. Somnambulistic activity may express a similar mechanism, that is to say, it is expressive of a regression to sub-cortical control, wherein inhibitory activities, characteristic of the cortex, are arrested. One “part” of the psyche is temporarily switched off and the activity is taken over by another “part” which is subconscious, autonomous, sometimes called “the shadow.”
Among alcoholics with psychoneurotic background we often observe a phenomenon of a strong urge to come out of the depression, out of the fluctuation, instability and conflicts associated with the disintegrated state. The tensions are so strong and so strongly they demand reduction that patients seek desperately some “disinihibitors,” of which the most accessible is alcohol. It is characteristic for the lower levels of the nervous system to act with greater tension. This power is evident in basic drives. Weak control and weak inhibition on the lower levels of the nervous system accounts for impulsive behaviour and psychomotor excitability.
Inability to achieve or reach a higher level of integration causes at times not only disinhibition tending to bring about integration at a lower level, but also disinhibition aiming at partial integration in an imaginary world, in a world of artificial, uncreative prospection. This may be observed among narcotic addicts. Conscious search for global solutions is an exceedingly difficult task while the actual situation may be un-
51
bearable. Hence it is easier to look for substitutes and immediate ways out of an emotional impasse.
The above-mentioned partial and pathological integrations and various forms of neurotic fixations (phobias, tics) are expressions of a partial disinhibition of cortical control with simultaneous partial subordination to the influence of sub-cortical centers.
3. Autonomic Disequilibrium
Basic phenomena of autonomic disequilibrium: Disturbances of equilibrium in the activities of the autonomic nervous system are manifested, according to Harvier and Chambruen as follows
1. Disorders of circulation: unstable pulsation, changing from slow to rapid; extrasystolis.
2. Respiratory disorders: unevenness of respiration, sighing, feelings of pressure in the respiratory system.
3. Nutritional disorders: fullness, unsatisfied hypersecretions, constipation, diarrhea.
4. Motor-vascular disorders: blushing, turning pale, erythema pudicum.
5. Secretional and excretional disorders: profuse sweating, waiting for the first and last drops while urinating, premature ejaculations.
6. Psychical disorders associated with disequilibrium of the autonomic nervous system: excessive activity and fatigue, excitement and depression, sadness and joy, optimism and pessimism.
These disorders are an expression of a variable and sequential activity of the sympathetic and parasympathetic systems, where one or the other is dominant at any given time. This state of affairs is analogous to the ambivalences and ambitendencies in the sphere of psychical activity.
Autonomic disequilibrium, especially when constitutional, is a lack of coupled control (synergistic control) between the sympathetic and the parasympathetic nervous systems. In conse-
52
quence a sudden shift in the direction of one or the other system is followed often by too quick, even violent, reaction in the other direction. Individuals with hyperactive thyroid, i.e. those with excessive activity of the sympathetic system, are subject to sudden onslaughts of fatigue induced by an over-reaction of the parasympathetic system. These people have to lie down at once, if only for 15 minutes, in order to restore their own peculiar balance of the autonomic-endocrinal systems.
4. Psychosomatic Disorders
Psychosomatic disorders basically can be reduced to hyper-functions, hypofunctions and dysfunctions of the autonomic system, within the domain of one organ or of a system of organs.
We find such local or narrow areas of disturbance, for instance, in spasms of the esophagus or pylorospasm (digestive system), and in spasmatic reactions of the glottis or trachea (respiratory system). They are also manifested in spastic irregularity of urination (“stuttering” in urination, intermittent urination), and finally in intermittent or premature ejaculation.
Readiness to spasticity in somatic neuroses may underlie the wandering spasticity, consisting of a periodic moving from one field to another, with attacks being focused at various points at various times. Readiness to spasticity has its constitutional root, among other factors in blood calcium deficiency.
It is sometimes the case that an increased excitability of a wider field diminishes the possibility of neurological “fixation” to a specific field. At other times the contrary is true; a widespread excitability localizes psychic tension. The tendency towards neurotic localization is more common among adults while the wandering is less common. Among children and adolescents prior to puberty the prevailing tendency is towards increased widespread excitability and wandering of symptoms. The majority of adult psychoneuroses are examples of localized or structurally condensed forms of psychic overexcitability. Children and adolescents are characterized by an enhanced excitability which is not locked into definite structures.
53
We find the phenomenon of neurotic weakening of action manifesting itself in various fields, for example in functional areflexia (extinction of palatal, pharyngeal or corneal reflexes), in hypesthesia (lowered sensitivity to tactile stimuli) or anesthesia (loss of feeling as in hysteria), and in hysterical sexual coldness. We recognize such hypofunction in “anorexia nervosa” (weakening of metabolism, exhaustion of the organism with concomitant high psychical efficiency) and finally in reactive depression (slowing down of psychical processes, lack of appetite, limitation in secretion of digestive juices, arrest of menstruation).
5. Sympathetic and Parasympathetic Tension.
Nervous individuals with enhanced psychic excitability can be observed to show certain symptoms pointing to an excessive tension of the sympathetic or the parasympathetic nervous system. In the case of an increased tension of the sympathetic nervous system we observe hyperactivity of the thyroid, fatigability, increased pulse and together with these physiological excitations we see mental alertness, initiative. In turn enthusiasm, joy and ecstasy excite the sympathetic system.
In the case of an increased tension of the parasympathetic nervous system we observe a decreased pulse, arrhythmia, slower rate of breathing, tendencies to contractions of some organs or systems of organs, and together with this physiological slow-down we observe lack of initiative, tendency towards analysis, incomplete attitudes, depressions, anxieties. And in turn, obsessions, sorrow and unpleasant experiences excite the parasympathetic system.
These tensions (sympathetic or parasympathetic) and correlated attitudes may occur alternately or form complexes. As a result we have a state of autonomic disequilibrium which is called amphotonia or dystonia.
There are many causes of internal disequilibrium. They may be strong emotions, stresses, grave psychical crises, or extreme fatigue. In consequence the first reaction might be an organized defensive reaction calling for increased tension (in one or another part of the organism). When the initial stimuli for
54
the defense are reduced or removed then the tension subsides with resulting disintegration on the territory of the autonomic nervous system. The organism returns to some equilibrium. Nevertheless a memory of the stress remains both organically and psychically and it is this which subsequently facilitates a nervous or psychic disintegration. This disintegration can be either positive or negative.
6. Emotions as Disintegrators and Integrators
According to Janet (1926) strong emotions have a disintegrating effect on the mind by diminishing its capacity for synthesis. They also have a disintegrating effect on the autonomic system. Thus we can assume that emotions act as disintegrators of the autonomic system.
Except for the studies of oxygen consumption, heart rate and skin resistance during transcendental meditation (Wallace, 1970) little is known of the responses of the autonomic system under such conditions as inspiration or ecstasy. Such conditions can be integrative and disintegrative at the same time; their integrating action consists of organizing the action of the whole psyche in obedience to a superior activity; they are disintegrating, also, in the sense that they exclude conditions of physical reality or of the immediate environment.
Now, an excitation of the sympathetic system causes psychical irritability and a tendency towards excessive activity; excitation of the parasympathetic system, however, causes anxiety of a depressional character, and feelings of oppression, sleepiness.
The disequilibrium of the sympathetic and the parasympathetic nervous systems and resultant psychic disequilibrium are causally related. Moreover, the excitations and depressions, irritations and anxieties occurring in individuals with a positive developmental potential evoke in them striving to overcome these reactions. Hence the inner conflicts which ensue appear to bring out a new factor in development, i.e. the process of hierarchization (see p. 39). The process of hierarchization introduces a direction in the conflicts by defining more strongly to the individual’s consciousness the levels involved in his con-
55
flirts. In this way occurs what one could call a psychologization of conflicts which started on the sympathetic-parasympathetic level now gradually move away from this level towards a more conscious involvement of feelings.
Vertical conflicts (because occurring between different levels) and autonomic disequilibrium are thus an expression of certain “laws” governing the transition from one level of development to another. In particular they can be applied to the transition from unilevel conflicts (i.e. those immediately translated into and expressed as sympathetic or parasympathetic disturbances) to multilevel conflicts (i.e. those which in addition, or even more predominantly or exclusively, involve conscious emotions).
We conclude
1. Disorders of the autonomic nervous systems, reactions against them (hypertonia followed by a hypotonia) and periodical balance awaken protective forces which are in the service of development. An individual seeking a way out of a situation often finds the solution by activating a more cortical and more frontal system of action rather than staying tied to psychosomatic reactions controlled by the autonomic nervous system (sub-cortical control).
2. These disturbances and disintegrations, these experiences and “thrusts of consciousness” would be—in neurological terms—a result of a transition from a subcortical to a cortical level, and from a lower cortical level to a higher cortical level (more frontal and more conscious).
3. In psychological terms this is a transition from the level of primitive integration to that of unilevel disintegration through the disequilibrium and disintegration of the autonomic systems. This unilevel psychical disintegration is then followed by a transition to multilevel conflicts and hierarchization which mark a high level of human dynamisms.
7. The Etiology and the Level of Psychoneurotic Processes
Global emotions, embracing the whole psyche, cause vago-
56
sympathetic dystonia. In some cases emotions are known to act primarily on the vagosympathetic system; in other cases, they act on the endocrine system (e.g. glycosuria, sudden halting of menstruation, secretion by lacteal glands). This means that emotions acting on the whole man cannot affect only the sympathetic or only the parasympathetic system but act on both of them and disorganize them both. (It is important to note that higher emotions have the power to organize the autonomic systems as a balanced ground in the service of development.) The stronger and more basic are the emotions the more they reach down to the “gut” level, i.e. to the endocrine glands seeking there some means of regulating tension.
It would appear more precise to speak of all these phenomena as psychoneuroses, provided that descriptive diagnoses include the major symptomatic areas, since observations may be made of a single individual who exhibits—at different times—dominant symptoms in various somatic areas while the participation of psychic factors may be evident to a varying degree. The symptomatological levels have to be taken into account beginning with the somatopsychic as the lowest, then psychosomatic, distinctly psychic, and finally the most conscious as the most complex and the highest.
The recognition of the level of the psychoneurotic processes is of primary importance. A high level of these processes will be less often associated with disorders of the autonomic nervous system. In this case we use the term “psychoneurosis.” A lower level of psychoneurotic processes will be often and strongly associated with disorders of the autonomic nervous system. In this case we apply the term “neurosis.”
Etiology of psychoneurotic disorders with a strong autonomic component is rather complicated. Emotions themselves may cause dispeptic disorders or increase symptoms connected with an already existing condition. An increase in pain of a stomach ulcer or its hemorrhage due to emotional stress is a well known fact. Similar cases may be observed regarding spastic conditions of the large intestine and general intestinal hemorrhages. Some individuals vomit in reaction to an emotional experience, such
57
as some unpleasant event, smell (cf. Case 1, p. 13 and ff).
Spasms which develop on the basis of special reactivity of the musculature of the stomach cause such responses as the above, according to Thomas (1929). The same individuals are often subject to diarrhea. Certain organs have either innate or acquired sensitivity, which is activated by emotional processes. Examples are ureter spasms, “stuttering” in urine rendering, intermittent defecation, excessive flow of urine after urination due to a lack of the final stopping spasm, halting of urine etc. Glycaemia and glycosuria increase in intensity as a result of moral shocks.
According to such investigators as Hayem and Thomas, in psychoneurotic dystonias eye pupils rapidly dilate and constrict, then dilate again. We are here concerned with motor-vascular hyperactivity, such that the patient reacts to the smallest emotional stimulus by either going pale or blushing, sweating or dermographia (reddening or whitening of the skin). Pulse acceleration is a common phenomenon; dyspepsia and diarrhea are common associates of fear. In serious anxiety conditions, swelling and skin irritation also are known.
In summary, neuroses are conditions of high (hypertonia) or low tension (hypotonia) of the autonomic systems. When these conditions of low and high tension alternate they create a dystonia or disharmony of the autonomic system embracing the whole organism. This dystonia affects the various systems in the organism simultaneously or consecutively.
Conclusions.
1. The autonomic nervous system has its own developmental potential which becomes manifest in states of disharmony of its component systems—the sympathetic and the parasympathetic.
2. Coupling between the psyche and the autonomic nervous system occurs under the impact of strong emotions.
3. Higher emotions enable one to transform these states of autonomic disharmony into hierarchic states and also to partially integrate them on a higher level.
58
8. Endocrine Glands
As previously mentioned, strong emotion has—according to Janet (1926)—a disintegrating effect (dissolvent) on the human mind thereby weakening its synthetic power and limiting its activity for some time. On the other hand we know that emotions have a considerable effect on the initiation and development of endocrine disorders [excessive thyroid activity, goitrous exophthalmia (protruding eyeballs), influence on the menstrual and lacteal activity or excessive secretion of adrenaline, histamine, etc.]. We also know that emotions play a large role in the genesis and development of neuroses and psychoneuroses. The autonomic nervous system works in close relation with emotions and with the endocrine glands. There were even attempts to develop a typology based on these three components (Jaensch, 1923). The pituitary body was sometimes called the endocrinological director cooperating with the autonomic nervous system. There is, therefore, a very close connection between emotional life, the autonomic system, and the endocrine glands.
Contrary to Janet’s ideas the role of emotions in relation to the mind, behaviour, and finally to the developmental processes is two-fold and only apparently antagonistic (in integration and disintegration); likewise with the endocrine systems. We can speak, then, of emotional, autonomic, and endocrine activities which may be either integrating or disintegrating.
One of the instances of endocrine disorders with serious consequences for mental development are several forms of infantilism. One is a mild hypogenitalism (subnormal development of genitals) which is often associated with a prolongation of the developmental period, giving rise to neurotic symptoms. On the other hand we observe cases of hypogenitalism and hypothyroidism (subnormal development of the thyroid) which are very often associated with mental retardation. Hypothyroid-ism occurs with myxedema and mongolism, both of which are forms of mental retardation. They frequently occur together with hypogenitalism in its negative form. Since there is weak psychic sensitivity and low intelligence, marked hypogenitalism
59
in combination with hypothyroidism gives the balance over to somatic life integrated on a low level. On the contrary such effects of hyperactive thyroid as enhanced excitability of affect and imagination combined with a non-pathological weakness of the sexual drive causes an individual to be astonished and disquieted with himself and also to be maladjusted in his environment.
Certain periods and conditions are more demanding of the thyroid; for example, the periods of maturation, climacteric, pregnancy, and various conditions of intoxication. We observe here the integrating function of the thyroid in periods of strong disintegration (maturation and menopause periods, anti-toxic activity, increased metabolism, and rise in body temperature).
9. Anorexia nervosa
Anorexia nervosa, so termed in 1868 by Gull, who described its most characteristic symptoms is very important as an example of the psychogenicity of disorders in organic functioning. Anorexia nervosa involves complete loss of appetite on the basis of which we recognize a pathological state of mind. Patients suffering from this illness exhibit a definite psychoneurotic personality combined with a special mental attitude of indifference and negation. This psychopathological condition may have a hereditary background and is often connected with emotional disequilibrium among adolescents or young adults, with such determining stimuli as the breaking of engagement or friendship, jealousy, unhappy marital relations, etc. There occurs in the individual a tendency to remain in this state by creating, for himself, a morbid pleasure in observing his own illness and in inciting other family members and friends to observe him and express their sympathy.
The basal metabolism connected with this disorder usually is very low (down to 40 percent). Low metabolism in a period of prolonged fasting permits these patients to remain alive. Mental and somatic activities of such patients often are satis-
60
factory as compared with the degree of their exhaustion and, in themselves, do not permit us to conclude that the origin of the sickness is organic. Pulse is slow, blood pressure is low and the temperature is subnormal; at time there appears a symptomless hypoglycemia and tendency to hypoacidity. Anemia rarely occurs. Sortels described 16 female cases in which the therapy consisted of psychotherapy and proper nutrition. There occurred nine spontaneous recoveries through the initiation of new, intense interests or hobbies. Girls and young women present the above disorder more often than do boys and young men.
Pathological elements (often of a positive developmental value), act as psychodisintegrators (loss of desire to live, suicidal tendencies, satisfaction derived from the influence of one’s own, serious effect on the family, self-observation as an object of pity). A return to good health through the development of new interests or through psychotherapy, without any thyroidin, insulin, or other pharmacological treatment, shows that the process of anorexia nervosa is originally developed in the psyche and not in the somatic area. If follows that there is a need to reactivate psychical integrators.
The described syndromes represent only a sampling of phenomena which are often regarded as pathological yet are very important for the positive development of man. For example a phenomenon analogous to anorexia nervosa is the self-imposed starvation (or fast) practiced by eminent men when they are facing insoluble antinomies. The fast becomes a method aiding in the search for a solution. Many psychically rich individuals experience these antinomies in a very deep and intense manner, the solutions appear contradictory, and ultimately there is only “suicide, gallows, or a goal higher and more beautiful than ever realized by man” as expressed by Weininger (1926).
Another example is the fact that psychoneurotic individuals, who possess mediumistic powers have strong biological urges after exhausting séances. It seems that they have to return to the condition of enhanced biological power and “normal” behaviour. This occurs as sudden upsurge of hunger or of
61
sexual tension. Dostoevsky’s self-disclosure (p. 51) is, another case in point. It appears that a sudden concentration of mental energy on a different level upsets the psychophysical balance of the organism and has to be later compensated. The higher, mental functions exert an inhibitory effect on the lower functions including the biological level. Control at any level can be exercised only by some means of inhibiting a process. It would appear that unusually strong for a given person concentration of mental energy on a higher level removes it from the lower levels so that in consequence the controls are unattended, producing the effect of a “descent to a lower level” just after the higher one was scaled.
10. Conclusions
1. In the course of evolution from higher animals to man, and from the normal man to the universally and highly developed man, we observe processes of disintegration of lower functions and an integration of higher functions.
2. The functions involved in this evolutionary process are all the emotional, instinctive and intellectual functions.
3. The establishment of the inner psychic milieu on a higher level and of an increasingly more human attitude towards the external environment requires the stimulation of higher functions and the inhibition of lower functions. This involves many kinds of sensitivity and excitability, numerous inner conflicts, emergence of multilevel inner forces, which can be called the dynamisms of the inner psychic milieu.
4. The disintegrating and integrating forces act on different levels as disintegrators and integrators of different mental functions.
5. The engagement of the higher mental functions in the transformation of the lower ones causes psychosomatic and somatopsychic disorders, neuroses of organs, hyper, hypotonia or dystonia of the autonomic nervous system. These disturbances come gradually under control in the general de-
62
velopment of the human species, and concretely in individual development.
6. Depending on the type of physical constitution, hormonal factors, psychological type, level and universality of development, social environment, we have in psychoneuroses either a dominance of psychical processes or of the processes involving the autonomic nervous system.
7. The manifestation of the interplay of the psychical and autonomic factors is enhanced psychic excitability (sensual, emotional, imaginational, psychomotor, and intellectual) when the processes occur at a medium level of tension. When the tension is higher then we have neuroses and psychoneuroses.
8. All these disturbances of the functions of the autonomic nervous system as well as the psychoneurotic “disorders” we regard as positive processes of development. This is especially true when internal conflicts and manifestations of psychical disequilibrium involve different levels.
9. Whether the disturbances of the autonomic and hormonal systems will be used positively or negatively in the development of the individual depends on the level and strength of his mental functions.
63
CHAPTER V
DISINTEGRATION AND PSYCHONEUROSES IN PERSONALITY DEVELOPMENT
1. Psychoneurotic Traits and Positive Mental Development
If we consider a person to be normal when reconciled with himself and his environment, that is to say, free in a period of months or years from more serious internal and external conflicts, then such individuals are less common in civilized societies today than those of increased psychic sensitivity, who are at the same time maladjusted to themselves and to their environment, and often torn by internal and external conflicts.
If to be free of conflict is “normal,” it is also normal to experience inner conflicts. In my opinion the second group is “more normal” because it has more distinct and more extensive developmental dynamisms as a part of their mental constitution than the “conflict-free” group.
Brun (1954) has said that a diagnosis of neurosis cannot be made exclusively on the basis of negative symptoms, but must include positive ones as well.” We wish to add that not only neuroses, but all states of nervousness, psychic sensitivity and psychic excitability have some positive traits bearing on individual and moral development.
We shall discuss these positive traits and their characteristics as follows
(1) Enhanced psychic excitability
(2) Tendency towards more of internal conflict and less of external conflict
64
(3) Psychosomatic sensitivity as an initial condition of disintegration
(4) Internal conflicts are not subconscious repression but conscious restructuring of different levels of the psyche
(5) Regression as a purposeful behaviour
(6) Infantilism
(7) Different levels of fatigue
(8) Quietude and solitude as necessary conditions of psychic synthesis and integration
(1) Enhanced psychic excitability.
An increased psychic excitability encompasses enhanced excitability of affect, imagination, psychomotor and sensual reactions, and intelligence (intellectual excitability). From these develops a wider spectrum of feelings, an increased field of consciousness, and a greater and more complex pattern of excitation and inhibition. Psychic overexcitability is one of the recognizable components of the developmental potential (cf. p. 6).
A person manifesting an enhanced psychic excitability in general, and an enhanced emotional, intellectual and imaginational excitability in particular, is endowed with a greater power of penetration into both the external and the inner world. He has a greater need to see their many dimensions and many levels, to think and reflect upon them. These forms of overexcitability are the initial condition of developing an attitude of positive maladjustment to oneself, to others, and to the surrounding world. One of my friends used to express it this way
“I am both disturbed by and attracted to the way I experience myself and the world. I have to see my experiences from near and from far, I feel the need to return to them, I have to see them in many dimensions, their limited and their expanded shapes.” One of my patients said this: “The images of people, experiences, problems, stand before me as ‘stages of evolution', as pictures or portraits, and each one of them—though reflecting the same phenomenon—gains in depth and complexity.”
65
Because the sensitivity (excitability) is related to all essential groups of receptors of stimuli of the internal and external worlds it widens and enhances the field of consciousness. The variety and cooperation between different ways of receiving these stimuli adds to this process. This sensitivity acting in the “unknown fields” of the inner and the outer worlds brings about a need for new experiences, for an uncertainty of experiencing, for hesitation and disquietude, which in general terms means a process coupling excitation with inhibition.
Excessive reactivity of nervous individuals to external as well as internal stimuli does not necessarily lead to trembling, psychomotor crises, or masturbation. Among individuals with a great wealth of feelings and creativity such excessive reactivity is conducive to the realization of their abilities, at least in the areas of thought and imagination. This depends very much on the type of overexcitability and on the level of psychic development. Individuals with enhanced emotional, imaginational and intellectual excitability channel it into forms most appropriate for them. They close themselves in the world of imagination, they isolate themselves in the outdoors or in their room, they read, they think or meditate, they go to see plays or films in order to see things other than those they tire of because of familiarity and lack of freshness.
(2) Tendency towards more of internal conflict and less of external conflict.
Affirming and denying certain influences from the environment and certain tendencies of the inner milieu often serves as a nucleus of discriminating activity in the making of conscious choices. A patient said: “I do not agree with myself, I condemn myself, I am ashamed of myself. I will not allow my “lower self” to choke my “higher self.” Some say that to have conflicts with oneself is bad. Nonsense. They make me grow, they make me understand others, thanks to them I am less in conflict with others.”
In case I in the second part of her biography we see that the patient reacted very strongly to external situations and that
66
she frequently transferred the center of gravity of her reactions onto herself (as a relation to herself). For instance in her fear of the possible coming of fear, in her fear of seeing in her own face in the mirror the signs of mental illness, she shows the transition from external conflict to an internal conflict.
In case 2 the patient became indifferent to external events, with the exception of the most brutal forms of behaviour around her, but transferred all her conflicts to her inner psychic milieu. They then became internal conflicts between the ordinary reality of life and the world of moral and transcendental reality. In case 3 we also observe that all conflicts take place in the world of inner life. They are invariably related to feelings of inferiority in relation to the patient himself, with a feeling of guilt, with a sense of an inner hierarchy of values, (yet universal) and a feeling of not having realized it to a sufficient degree. In case 4 we observe almost exclusively external conflicts. In response to these conflicts there are phobias and obsessions. The incapacity to make the transition to developmental inner conflicts is directly related to the absence of hierarchical elements.
(3) Psychosomatic sensitivity as an initial condition of disintegration.
A lack of equilibrium and a lability of one’s own inner psychic milieu is expressive of disintegration, which is found at the root of conflicts between higher and lower tendencies. The “somatopsychic relations” by causing functional difficulties, collisions between conflicting “sides,” bring attention to these states, and consequently to what is happening inside the individual’s mental and emotional structure. This is how attention is brought to the events of the inner psychic milieu. More extensive discussion of this subject is contained in Chapter 3 and 4.
(4) Internal conflicts are not subconscious repression but conscious restructuring of different levels of the psyche.
Conflicts and conscious and unconscious repression do not
67
necessarily derive from sexual tendencies as primary factors, but rather express a multiple intra-level process of inhibition of primitive tendencies, in favour of gradually increasing higher psychical processes.
According to Sherrington (1961) man’s cultural level can be correlated with the amount of inhibition over the amount of excitation. If there is more inhibition and less excitation then such a man is culturally higher than one exhibiting the reverse. Sherrington showed that if the higher levels of the animal’s brain are dissected out then the lower levels (the spinal cord) become more excitable. These inhibitions either can be a direct result of an active inhibitory process or they can result from the excitation of higher functions which indirectly inhibit lower functions in a given area of psychic activity.
I have indicated that such indirect inhibition or damping of lower functions may be applied to all functions in development. This can be found in clinical experience. One of my patients said: “When I recognized how easy it is to hurt people by lack of attention and care toward them I resolved to make the effort to avoid rash decisions, to avoid feeling offended, disliked, or simply being stubborn, in order not to base my reactions on such feelings. Otherwise it would be as if I looked through dark and unwashed glasses.”
The restructuring of different levels occurs through inner psychic transformation. A characteristic example exists in case 3 where there is a continuing evolution of a hierarchy of values, of expecting more and more from oneself, and an increasingly clearer identification with the personality ideal.
(5) Regression as a purposeful behaviour.
Retrospections and regressions to the past, to childish tendencies, are not necessarily expressive of a repressed “libido” (especially in the form of Electra, Oedipus, castration and other complexes) but rather of a need to return to a most happy period, to a period of intense development from which to draw new energy. Equally often these reactions represent prophylactic stratagems called in to handle future conflicts with the external
68
world, as well as in the inner world (prevention of nervous breakdowns or suicide).
It is in fact a general principle that in order to achieve some degree of inner integration and stability we must at times remove ourselves from active life and retreat to the world of dreams, friends, family, nature, solitude, creativity, theatre or film. We have to leave for a while our actual reality and return or transpose our “longing heart” to the past, to dreams, or to whatever “otherness” that brings us repose.
The tendency to “fall into sickness” is an escape from people, from an external milieu, and from unsolved problems. It is very often related to hypersensitivity of consciousness. For some people it is the only available means of protection—taking cover before the brutality of life.
(6) Positive infantilism.
Some theories of neurosis (e.g. those of Masserman, Mazurkiewicz, Zajaczkowski) postulate that the immaturity of emotions and drives which characterizes infantilistic individuals may also characterize psychoneurotics.
On the other hand we know from clinical examinations and tests that some infantilistic individuals exhibit a high level of intelligence, emotional sensitivity, refinement, intuition, creative abilities, and capacities for heroism and self-sacrifice.
Heroism and self-sacrifice are correlated in these cases with sincerity, suggestibility and lack of calculation.
Such infantilism is often found in psychoneurotics, especially in psychasthenics, but also among outstanding individuals in art, science, and sometimes in public service. Here belong Mozart, Beethoven, Chopin, Keats, Musset, Slowacki, Shelley, Rousseau, Chagall, Walt Disney, and thousands of others.
A lack of appreciation of infantilism is usually based on observations of its “negative” aspects, such as wavering attitudes, excessive affective excitability, sensitivity and excitability of imagination, feelings of inferiority, shyness, “immature” behaviour, impracticality, excessive intimacy and sincerity, lack
69
of adjustment to reality, sexual immaturity expressed in weakness of the sexual drive, tendencies towards platonization of sexual feelings, fears and disturbances in sexual tension, or even feelings in a young man towards a woman as a friend, a lover, and mother all in one person.
Infantile characteristics are physically registered in facial expressions, in a direct and sincere smile, in refined, gentle movements and gestures (often seen as feminine bodily characteristics in men, or boyish ones in women). Infantile characteristics can also be observed in inhibitions of behaviour or suggestibility.
One may well ask: in what respect are they immature? Is it true that sensitivity, refinement, and remoteness from practical life indicate immaturity of emotional and aspirational structure, or only an immaturity in relation to a narrow material reality, to a low level of daily events and deadly routine? I believe that we may answer this by saying that individuals with infantile traits are often adjusted to a “reality of a higher order.” They are more developed verbally and conceptually than in matters of practical importance. Their basic drives are less strong. In the terminology of Janet (1926), we may say that they have weakly developed reality functions with respect to an average social milieu and its requirements. These individuals have an extended, as it were, period of maturation, which secures for them a richer and more universal mental development. An extended period of maturation lasting over years of so-called impracticality, puts them in a position favourable for the achievement of a high level of psychic development, in comparison to so-called normal individuals. One of the best examples of extended and unfinished maturation is Michelangelo (Dąbrowski, 1937; Dąbrowski, 1967).
By higher level of psychic development we mean a behaviour which is more complex, more conscious and having greater freedom of choice, hence greater opportunity for self-determination. By a lower level of psychic development we mean a behaviour which is less complex, more primitive (i.e. more con-trolled by basic drives), more egoistical and less conscious. In such behaviour one cannot properly speak of self-determin-
70
ation. These levels of behaviour have been more extensively characterized elsewhere (Dąbrowski, 1970).
Infantilistic individuals, often endowed with much charm, freshness, spontaneity and richness of imagination-besides helplessness in practical situations-often exhibit lack of coordination of movements. The fact that a newborn human baby is far more developed in its ability to move its limbs than a new-born animal is well recognized. But it takes much longer for the human baby to achieve dependability of its movements and it never reaches the proficiency characteristic for some animals. Evidently the human cortex is involved in other processes. The greater the role assumed by the cerebral cortex in motor development, the more disorganized and helpless are movements of a newborn baby, and the more psychic and motoric variety and richness is found in adult individuals. Infantilistic persons often exhibit limited psychomotoric fitness, which is being integrated only with difficulty during their whole life, and this very condition of psychomotor disintegration must be considered in numerous cases as a symptom corresponding to a development of higher functions, with concomitant neglect of psychomotor functions.
(7) Different levels of fatigue.
The excitability and fatigability of neurotics, but especially of neurasthenics and psychasthenics, does not uniformly extend to all spheres of activity. This fatigue may be negligible in some activities, and very considerable in others. Excitability and fatigability in psychoneurotics may be a positive or negative phenomenon depending on the concrete activity involved. On the other hand, the same psychoneurotic who is subject to fatigue and inaction on a lower level of functioning may show no fatigability in his creativity, which is a higher level of functioning.
Proust, for instance, suffered unbearably when he had to take care of his household duties, his finances, etc. Nevertheless, he was capable of sustained and systematic hard work of writing. It gave him a great creative satisfaction Kierkegaard, Una-
71
muno and Chopin were very similar in this respect. We can observe a similar phenomenon daily in very talented children who quickly tire, become exhausted under conditions of imposed school instruction but can without fatigue spend long time playing with things they like.
(8) Quietude and solitude as necessary conditions of psychic synthesis and integration.
Contrary to the opinion of Brun (1954) that night is the enemy of psychoneurotics, we find that often such individuals are particularly creative at night since then their ability for concentration is unhampered. The night by its quietness and freedom from being disturbed releases their ability for synthesis, meditation, and internal transformation. We see this phenomenon often, especially in such writers as Balzac or Kafka, who wrote at night. Most young, intelligent and creative people with psychasthenic traits spend time late at night working creatively or discussing philosophy and moral questions.
The thing in question here is not only quietude and solitude at night but also during the day through short moments of isolating oneself from external stimuli and transition to the reception of internal stimuli. Such quietude and solitude in order to open oneself to internal stimuli is necessary for most writers, poets, musicians, painters, who also show strong components of introversion, hierarchization of values and unfolding of their inner psychic milieu. Such states of isolation occasionally take the character of a positive, one may say even healthy and desirable autism. Such autism is not a rigid psychical organization but a temporary complex of behaviour serving to put oneself in order by closing off the external world and plunging into meditation. Such autistic periods are at times necessary to improve relations with others and to raise the level of empathy. For example, Socrates spent many hours in solitude deep in thought and for this some considered him a sage and others a madman; Gandhi observed a day of silence once a week. The same type of behaviour is found among saints of all
72
nations, yogis, and others having the recognized or unrecognized distinction of advanced development.
* * *
All the above mentioned mechanisms are expressive of the process of disintegration which may be more or less universal and may take various forms. These are the mechanisms of an inner loosening (disintegration) which may last for a more or less extended period of time. It is our view that such psychic disintegration contains dynamic, creative elements and leads ultimately to personality synthesis, or what we have called “secondary integration.” According to Proust (Du Côté de Guermentes) all great things we have we owe to neurotics. They are the ones—and not others—who have originated religions and created masterpieces. The world may never know how much it owes them, and especially how much they suffered to produce it. We glory in their divine music, their beautiful paintings and thousand subtleties, but we do not know the price they paid in sleepless nights, crying, spasmodic laughter, asthma—and the ever-present fear of death, which is the worst of all.”
With these notions, and with my own, Abély (1959) also is in agreement: “I met in my life, especially in artistic milieus, nervous individuals of great talent, who, happily, remained such. Neyrac described “the anxiety of Saint-Exupéry.” He said something along these lines: “This fear was of a special kind. It had some potential for elevation in personality development. Such anxieties are instrumental in raising one to a higher level, and the psychiatrist should approach them with prudence and respect.”
2. The Role of Polarity in The Process of Positive Disintegration
We frequently find in psychoneuroses outstanding examples of mental ambivalence. An easy excitability and depressiveness, considerable sensitivity to the problems of others together with irritability and withdrawal, a periodic tendency to explosiveness followed by slowing down of emotional processes, likes and dislikes expressed through changing and contradictory atti-
73
tudes towards the same persons-are often syndromes of psycho-neurotic character but of a rather low level of mental functioning. An attitude of affirmation interposed with negation, positive and negative viewpoints taken in turn with regard to the same values, opinions and people, is what is called a polarized attitude. It is characterized by emotional fluctuations between pleasant and unpleasant, between joyous and sad. It is similar in meaning to ambivalence.
We can say that in psychoneuroses we deal with “polarizing. disquietude” directed towards the negation of stereotype. We also find in relation to these properties a facility for expressing mixed feelings. Loosening up and even disintegration of his cohesive (even rigid) structures and complexes of activities permits a person to simultaneously experience qualitatively opposite emotions. This may be, for instance, an experience of “joyful sadness” because one cannot fill the actual, momentary events with simple and pure joy since one looks back on happy moments that never returned and one also looks into the future to new burdens, responsibilities and obstacles. This is retrospection and prospection. It may appear as nothing but neurotic gloom, nevertheless, we consider it a necessary step in expanding one’s horizon of awareness. Here belong mixed feelings of sympathy and resentment towards the same individuals, or the experiencing of “smiling through tears.” Just as there can be simultaneous excitability and depression, syntony and estrangement, so too, simultaneous attitudes of excessive prospection and retrospection are an expression of a widening internal and external reality and of growth in the experience of life.
The fluctuation of mood is not only the most important trait of the cycloid type (Kretschmer) which in its pathological form appears as the manic-depressive psychosis, but occurs also in individuals endowed with enhanced sensual and emotional excitability. The fluctuation of mood appears also in psychoneurotic infantilism and in hysteria. In both these syndromes we observe capriciousness and delicateness, suggestibility and stubbornness, psychical over activity and indifference, and even tendencies for immobilization and autism.
74
In hysteria we find besides this also other forms of polarization, such as excessive fatigue, suggestibility, hypnotic states, excessive sleep, or even hysterical paralysis as a pathological form of immobilization aside with excessive stimulation, resistance to fatigue, and so on.
Likewise in the manic-depressive psychosis we have as one pole excitation, excessive mobility, quickness and richness of associations, euphoria, facility of relating to the environment, and as the other pole apathy, depression, slow tempo of reactions, feeling of inferiority, etc.
These states may be the outcome of a necessity to change a state of excitement into a state of depression and vice versa, to change from an excessive involvement into immobility. This may be necessary in order to repair the loss of energy.
We find in cases of hysteria that sometimes a patient develops an excessive need for attracting attention by being dramatic, as if he were on stage, by eccentric dress, and if this does not suffice, he will express this need by immobility or hysterical paralysis.
A hysterical “flight into sickness” during a difficult situation is just the application of one of the accessible poles of the polarization tendency. A narrowing of the field of consciousness which characterizes a very distinct hysterical condition is closely related to the acceptance of a unipolar attitude, compatible with only some type of stimuli and the exclusion of others. The other pole is excessive sensual and psychomotor excitability, a showing-off behaviour. It was Janet who recognized this “narrowing down of the field of consciousness” to only one kind of stimuli, one kind of experiencing, one kind of attitude. I have known a case of a small girl who suffered the same pains as her hospitalized father. She so much loved and identified with him that her consciousness was narrowed down to experiencing the same kind of condition as her father’s.
Symptoms of suggestibility and autosuggestibility are an expression of hysterical mechanisms, as in the examples given above or in case 7. These mechanisms are mobilized in order to realize or form a direction along which the individual can
75
find, more or less consciously, his own lifestyle, whether normal” or “neurotic.”
Under the pressure of these occurrences there is an increasingly more urgent search for “developmental” way out of the situation, for a channeling of the pressures “up.”
In the process of unilevel disintegration, slowly advancing to multilevel disintegration, the hierarchic organization advances and so does the increasingly conscious role of the disposing and directing center. This center embodies in itself the programming, planning and organizing of behavior. It determines particular acts of behavior as well as its long range direction. In primitive behavior, which we define as one controlled by basic drives, the disposing and directing center does not appear as a conscious activity separate from the basic drives. It is only at a more advanced level of development that a conscious direction and conscious developmental choices begin to appear together with projections into the future (“who will I be”) that we can speak of the disposing and directing center as a dynamism.
76
CHAPTER VI
PSYCHONEUROTIC SYNDROMES ACCORDING
TO THE THEORY
OF POSITIVE DISINTEGRATION
The developmental process in which occur “collisions” with the environment and with oneself begins as a consequence of the interplay of three factors: developmental potential which is positive for the most part (different forms of over excitability), an influence of the social milieu, and autonomous (self-determining) factors. With time there is an increase of excitability, inhibitions, inner conflicts, external conflicts and tensions.
Depending on both the strength of the developmental potential and social influence, the development may be arrested in its course at the stage of unilevel disintegration for a long time, or it may fairly early enter into the stage of multilevel disintegration. Accordingly, we shall have different rates of development and different prognosis. In consequence, we will encounter “higher” and “lower” levels of psychoneuroses, some more linked with the disorders of the autonomic nervous system and organic functions (psychosomatic disorders), some more linked with higher levels and higher emotions (as in psychasthenia or psychoneurotic anxiety). We will observe a wider or a less wide globalization of the psychoneurotic process. Every phenomenon has thus to be examined in its “depth” and its “width,” i.e. horizontally and vertically. Development with the participation of psychoneurotic processes proceeds in relation to these two vectors.
1. The Expression of Psychic Overexcitability in Psychoneurotic Processes
In an earlier section (Chapter 1, Section 4), devoted to the role
77
of the developmental potential in psychoneuroses, it was pointed out that this potential is discovered in different forms of enhanced excitability, in the nuclei of the inner psychic milieu, in special interests and abilities. The development of the inner psychic milieu is strictly related to the activity of autonomous and authentic dynamisms such as the third factor, subject-object in oneself, self-awareness and identification with one’s own development.
The relations and interactions between the different components of the developmental potential give shape to individual development and control the appearance of psychoneuroses on different levels of development.
(1) Limited developmental potential.
In the case of enhanced sensual excitability but without a more pronounced presence of hierarchic and autonomous dynamisms we observe the development of hysteria on a low level. Its characteristic form is a characteropathic hysteria expressed through primitive playacting, lying, intriguing and the like, There is also sexual excitability as a response to feeling threatened, need of defense, or the need to reduce tension.
In the case of psychomotor overexcitability without a more pronounced participation of hierarchical dynamisms we observe functional hyperkineses, tics, psychomotor crises, wanderlust.
In the case of emotional (affective) overexcitability we observe emotional crises with not much awareness, inhibitions or aggressions, primitive fearfulness. We observe also phobias, affective perseverations, hypochondriacal and neurasthenic reactions.
In the case of imaginational overexcitability we observe waking dreams, unconscious obsessions of imagination, symptoms of psychoneurotic autism, hypochondriacal and neurasthenic symptoms with strong component of imagination.
In the case of enhanced intellectual excitability we observe excessive questioning, excessive analyzing, isolation, introvertization, weak emotional contact with the environment, in other words a marked asyntony.
(2) Strong developmental potential.
The forms of expression of psychic overexcitability described
78
above are those that do not have a strong developmental potential. Those that do take on more complex forms. When the developmental potential is strong then a new and very important factor comes into play, namely hierarchization. This is the beginning of the development of a multilevel inner psychic milieu.
In the case of sensual overexcitability the developmental tensions, i.e. internal and external difficulties, may push a given individual towards conflicts between his primitive sensual and sexual tendencies, and his sexual needs of higher level. This may take the form of hysterical conversion, localized neuroses, nervous stimulation, or sexual “frigidity” during intercourse. We may observe an excess of indirect sensual needs such as for touching as a way of compensating for the feeling of guilt related to sexual frigidity.
In the case of psychomotor overexcitability we observe more complex perseverations of movements, as for example, counting telephone poles, counting steps, fear of surprise, need for spastic expression, excessive talking, impulsive walking, taking walks to release tension, frequent movie-going, etc.
Psychoneurotic processes stemming from emotional overexcitability take the form of depressions related to feelings of inferiority, of shame and guilt, fears of responsibility, fears of death. Suicidal tendencies and suicides are not infrequent.
Psychoneuroses based on enhanced excitability of imagination are often characterized by deficiency of the reality function on a low level (everyday needs and occupations) but its strength on a higher level (life of inspiration, ideas, creativity and experience of other dimensions of reality), imaginational obsessions, richness of dreams, ideas, inventions, creativity, which in the eyes of others usually have an “unreal” character.
In the case of intellectual overexcitability on this level we observe an “intrusion” of affective and imaginational tendencies into intellectual activities. The intellectual processes thus become more complex and enriched. In psychoneurotic processes there are perseverations as to the “negativity” of the intellect, fears of synthesis, search for synthesis, fears of intuition, and a need of intuition. There are obsessions of responsibility and obsessive fears of one-sidedness.
79
(3) Strong developmental potential with marked autonomous dynamisms.
When the processes of hierarchization move from the phase of spontaneous conflicts and un-programmed searches for solutions to a phase of greater role of consciousness and organization, then the psychoneurotic processes reach a different level of expression. This level of development is reached only when the autonomous components of the developmental potential are very strong, and that means a high level of self-awareness and self-determination.
In the case of sensual overexcitability we now encounter structural complexities. The components of affective, imaginational and intellectual overexcitability push sensuality away from its dominant position. Hysterical tendencies are transformed into playacting on a high level, into suggestibility towards stimuli of high level; there is a development of empathy, contemplation, even ecstasy. There is a development of new attitudes. such as enthusiasm, enchantment, asceticism, striving towards sanctity.
Psychomotor tendencies are inhibited and transformed. There is a cooperation between affective, imaginational, intellectual and psychomotor components of overexcitability. It is expressed in a zeal for organization, planning and programming. There is a need for deeds which may give rise to psychomotor obsessions of existential and organizational nature; or to tendencies to create great works. This is a psychoneurotic trait of an excess of activity developed on the basis of “internal psychomotricity.” Saint Paul and Saint Theresa of Avila are good examples of this inner pressure for deeds on a large scale.
Enhanced emotional overexcitability takes the expression of a need for humility, asceticism, depressions, existential anxieties, affective obsessions in relation to responsibilities.
On this level psychoneuroses express not only individual phenomena and experiences but more and more strongly relate to other human beings. This comes about through compassion, genuine interest in the conditions of the lives of other people, their suffering, their existential difficulties. One could say that
80
these psychoneuroses arise from an excess of empathy and from an excess of authentic attitude towards another (“Thou”).
In the case of predominance of imaginational overexcitability the psychoneurotic processes are also expressed in depression existential anxieties and obsessions, empathy, etc., but perhaps with lesser intensity of symptoms than in the case of emotional overexcitability.
These forms of psychoneuroses have always to some extent open possibilities of “self-relaxation” in the world of imagination or dreams with the participation of enhanced affective and intellectual activity. This allows an easier systematization and easier finding of solutions to difficulties related to lower levels of reality than those proper to this type of psychoneurosis. This level of development (which elsewhere we call the fourth) is so universally involved in the reality of a higher order that the individual moves there with considerable ease whether it relates to his own individual problems or to the problems and difficulties experienced by others. The imaginational component makes it easier to move in the complicated world of tensions, depressions, or obsessions. For these people the gate into another reality is just wider and more open.
Psychoneuroses with a predominant component of intellectual overexcitability are characterized by a greater systematization of experiences, and hence by a greater need of rationalization. There are also depressions, obsessions and anxieties. One has to keep in mind, however, that on this level the types of psychic overexcitability are invariably mixed being composed of several forms of overexcitability, primarily affective and imaginational. Philosophical obsessions, obsessive criticisms of scientific theories, depressions related to the disillusionment that science is not capable of answering the most fundamental problems of life, are rather frequent. No infrequently one encounters also obsessive intellectual attempts to find scientific answers to the questions of life and existence.
The following four cases will serve as an illustration of different psychoneuroses and different levels of psychoneurotic processes.
81
2. Case 6
S.M. was 23. He studied history and theory of art at the university and at the same time he attended the Academy of Fine Arts in Warsaw. Prior to that he changed his major subject several times.
For some years he had symptoms of excessive nervous excitability, he was depressed and began to think of the danger of mental illness. In a few months his condition became more aggravated. He went through periods of “mental spasms.” On one hand, he considered himself normal; on the other hand, he thought of himself as one overly concerned with moral issues.
He went to look at the places of execution (he lived in Warsaw after the Second World War); he experienced the tragedies of the past as something of actual validity, something authentic. He was hypersensitive to blood. He thought that those who pass away are being consecrated for him, so that he becomes responsible for the continuation of their lives. At times he felt that such experiences were dangerous, but something attracted him to them. He was often concerned about the moral value of art. He separated the domains of higher value, which had for him a most real meaning, from those domains of lower values with which he was in mental warfare.
Moral problems were of such fascination for him that he wanted to discontinue his studies in art. He was interested in the fate and destiny of man, in his crisis in medical, psychological, moral, educational, or legal aspects. He experienced deeply and adversely, any such attempts at new types of education which, in his view, were contrary to human dignity. He experienced these confrontations somewhat like shocks.
Examination, internal and neurological:
Wide eye pupils, strong eyelid trembling, blood pressure 100/130, red dermographia increased. Chwostek on both sides strongly positive, abdominal and muscle reflexes increased, oculocardiac reflex inclined to arrythmia.
82
Psychological-psychiatric examination:
Outstanding affective and imaginational sensitivity, fairly well-developed ability for transposing psychic experience onto the autonomic nervous system. Strong preponderance of higher levels of emotional life, considerable capacity for inner psychic transformation (when he came for treatment he was looking for help in changing himself, he understood that individual development requires universal attention to human values, and that it cannot be achieved alone). Inner psychic milieu distinctly in hierarchical order. Outstanding intelligence with more facility for the theoretical than the practical. Some original traits in thinking. Multidirectional abilities. Reality function well developed at higher levels of mental life, and poorly developed at the lower, everyday level.
Interpretation:
His inner milieu is built on an authentic hierarchy of values, where the dominant elements are the highest dynamisms of mental life. The dynamisms “subject-object” in oneself and the third factor are manifested by his careful observation of the changeability of his own states, by their evaluation, and by his selective attitude (positive to some states, negative to others). This is also manifested in his attitude to his own artistic work. Moral values which he put on the highest level fascinated him, so that he subordinated all other values to them (thus placing his disposing and directing center on a high level). His highest values were global and humanistic. The whole organization of his life was based on these dynamisms together with constant retrospection and prospection in relation to himself and to the world around him. All these characteristics, with concomitant decrease in activity of the instinct of self-preservation and strong multilevel disintegration (feelings of responsibility, “excessive” syntony, dissatisfaction with himself, an attitude toward himself as object and toward others as subjects, the third factor, definite localization of disposing and directing center at a higher level)—all these indicate the development of insight, of a wide scale
83
and deep penetration of aims and firm non-adjustment to lower levels of reality.
Clinical diagnosis:
Psychasthenia with “pathological” empathy. An individual of higher psychical structure and highly developed mental functions. Good prognosis.
Treatment:
It is difficult to suggest here a specific program of treatment. Rather, a program of self-development and autopsychotherapy is advisable. It is important to have the patient realize the whole importance of his own development, to help him in a more universal personality growth, and in the control of his overly intense emotional reactions. He needs to develop a greater understanding and capacity for a more balanced view of the constellations of lower psychosocial level with some compassion for those who are morally endowed but to a limited degree.
S. M. has outstanding multidirectional abilities, high sensitivity, and distinct empathy. The hierarchy of his inner psychic milieu is marked by dominance of the highest dynamisms of mental life, creative ability, and considerable capacity for inner psychic transformation (he shows a constant need of self-development, of increasing his insight, of enlarging his understanding of others).
On the other hand, he demonstrated disproportional development of certain dynamisms of the inner psychic milieu, such as dissatisfaction with himself, feelings of inferiority with respect to himself, the dynamism “subject-object” in oneself, and also the third factor. In clinical diagnosis it may be considered that S.M. suffered from psychasthenia retaining his reality function at a high level (refinement, and moral concerns of universal nature) but with weakened reality function at a lower level.
S.M. represents an outstanding, positive personality development at the level of advanced multilevel disintegration. He is very sensitive, with increased affective, imaginational, sensual and mental activity. He manifests a strong attitude of meditative empathy and responsibility towards others. He also demonstrates
84
a highly educated awareness in the service of a well-developed moral personality. He has distinct creative abilities. S.M. represents, in the great majority of his symptoms, positive nuclei of personality formation, nuclei which are being actively developed and realized.
Is this case of psychoneurosis a case of illness? We can say that S.M. is definitely healthy, because he realizes his own model - norm or personality standard. His maladjustment to lower levels of actual reality, but adjustment to reality of a higher level, his empathy, his emotional tension, plasticity and creativity, and his responsibility and moral sensitivity are an expression of the acceleration of his developmental process. This is also demonstrated by the strength of the main dynamisms of his inner psychic milieu. At the same time we observe weakening of his instinct for self-preservation.
In a case like this I never recommend a “psychiatric treatment.” Should this man take up a professional psychiatric or clinical career, he would have exceptionally good chances of healing others, because of his great creative potential, empathy, psychical responsibility, insight and flexibility. One could only venture to give him some advice, on the basis of a global diagnosis of his rich personality, as being well on its way to advanced development. This development may be modulated through increased awareness and self-awareness, through a better under-standing of his own mental condition, through autopsychotherapy and periodic contacts with a psychologist or psychiatrist of high psychic maturity and capacity for an understanding of such individuals and their developmental processes.
3. Case 7
Z. S. was 38. She came with the complaint of nervous exhaustion, feelings of psychic weakness. For her every strong unpleasantness or stress resulted in weakness. Yet she felt a need for an active life and liked activity and initiative.
At times she had headaches, heartache, nausea. No disturbances of digestive tracts noticeable. For some months she has experienced something new coming over her organism, a sens-
85
ation new and strange to her. She lacked appetite and nausea was common. She believed that she was pregnant, but there was no physical ground to suppose it. She did not feel mentally ill, maintaining that she could control herself.
She had a love partner, but was not sure of his attitude. She could not be sure whether his feeling for her was genuine. She did not recognize spiritual relations without a ground of “concreteness.” In her partner she recently noticed an attitude “of prudishness, previously absent. Because of the unnaturalness and lack of sincerity in the patient it was difficult to establish to what degree their sexual life was normal.
Lately, she often had a recurrence of nausea, with the supposition that she might be pregnant without sexual conception She asked the physician to treat and examine her increasing abdomen. She wanted to see a gynecologist. She wanted to get married, especially in order to conceive a child, feeling a great desire for motherhood.
General and neurological examination:
Regular build. Low blood pressure. Abdominal muscular reflexes much increased. Chwostek positive on both sides, red dermographia extended.
These results indicate a generally enhanced psychical excitability, particularly sensual, tendencies towards “psychic spasmophilia.” The strongly increased abdominal reflexes may indicate that certain problems are localized in the genital and digestive systems.
Psychological and psychiatric examination:
Rather sure of herself, authoritarian, weak inhibition, marked ambivalence. Medium level of intelligence, more practical than theoretical. Intelligence in the service of strong basic drives, rigidity of thinking (stereotypy). Suggestibility, lack of criticism towards herself, excessive and facile transfer of psychic tension on to the body (autonomic somatization), weak inhibition with strongly enhanced excitability indicate absence of inner psychic
86
transformation. Her disposing and directing center at the service of the rather primitive drive to get married and be a mother. Besides objective, rather strong magical thinking (she believed herself pregnant). Poor hierarchization of values. Symptoms of slight disintegration of unilevel character but in general closer to primitive integration; preponderance of integrative elements.
Interpretation:
An individual integrated at a rather low level with some symptoms of a primitive unilevel disintegration. Moral attitudes based on a sense of duty and social norms, but rather primitive and weakly controlled. These tendencies and moral principles, are under the pressure of basic drives.
As a teacher with good experience and background and a person observing her religion, she followed the moral principles of right and wrong and appeared to differentiate them well. Nonetheless the pressure of the sexual and the maternal instincts was so strong that they manifested not only in pharisaical dosages of sexual contact but also in her magical thinking going far in the direction of believing with certainty that the outcome of these sexual contacts, namely pregnancy, was an irreversible fact.
Strong pressure of sexual and maternal needs, (self-suggestion of pregnancy) giving rise to magical thinking and action, approaching hysterical conversion. Strong tendency for the transmutation of the psychical into the somatic. Persistently false perceptions of her abdomen being enlarged and that her pregnancy was real indicate that her psychological processes were very much tied up in the somatosexual area.
Descriptive diagnosis:
She displayed excessive psychical sensitivity since childhood. Her disturbing experiences led to a state of anxiety and obsessions. Her repressed wishes acted through the subconscious, e.g. she believed herself pregnant with all the evidence to the contrary and tried to convince her lover and her physician. She feared that her lover would refuse to marry her. This created a fear of psychical shock experienced each time she found evidence
87
that her lover was not inclined to get married. She showed definite withdrawal (ekklisis). The case shows clearly that there was no ability for inner psychic transformation, i.e. no ability to accept and work out—even if only partially—her difficulties. In consequence she was in no position to handle the magical elements of her anxiety. She therefore possessed numerous components of a somatic neurosis since her body was the only available territory where to localize her unresolved difficulties.
Clinical diagnosis:
Symptom complex approaching hysterical conversion reaction.
Prognosis:
Doubtful in the sense of positive development.
Treatment:
The patient needs to be persuaded that her behavior will bring no results, and that her “wishful thinking” will not make her pregnant. It is necessary to help her realize that she needs to find her own independent meaning of life, and that this will help her to establish a relationship with her love partner without making her dependent upon hum. She needs either to marry her love partner, or to give up marriage and him. Another possibility, much less likely, would be for both of them to live together without legalizing it. The latter solution would have to be arrived at as a result of very clearly defined and realistic understanding between them of the conditions and consequences of such a decision. If she decides to get married, and marriage was possible, it would be necessary to give her help in organizing her married life, especially in difficult for her periods which would inevitably follow.
4. Case 8
M.L. was a man 40 years old, occupying a prominent scientific position. He came in because of periodic headaches, shortness of breath, heartbeat and disturbances in the digestive tract,
88
evident in occasional migrating pains and digestive irregularities. With varying intensity, he has suffered these symptoms for several years.
Developmental history:
His family (parents, grandparents, cousins, etc.) showed no history of mentally abnormal behavior (psychosis, retardation or the like).
The patient was the only child, educated in a soft atmosphere, yielding to his pleasure. He was egocentric and had an exaggerated notion of himself. On one hand he strived for perfection, on the other hand in his sexual relations with women he abused them.
General and neurological examination:
Moderate trembling of eyelids and hands, excessive muscular but especially abdominal reflexes; increased and extended red dermographia. Blood pressure 155/100.
The results of this examination indicate considerable general nervousness of the psychomotor, sensual and emotional type, marked cutaneous sensitivity (dermographic reaction). Abdominal reflexes excessively intense in his case may indicate his susceptibility to disorders of internal organs situated in this area. One would thus expect in this patient neuroses of the digestive system, most likely of the spastic type.
Psychological and psychiatric examination:
High level of intelligence, mainly theoretical, though in some areas practical side was fairly good. Symptoms of magical thinking (for instance in the fact how important to him was the ceremonial procedure of festive occasions in his church or in his everyday routine). Preponderance of introvert tendencies, egoistic and egocentric in character. On one hand he exhibited the so-called “spiritual desires,” and on the other hand excessive care for his own comfort and pleasure. In his religious practice ritualistic observance was dominant. He used cere-
89
monial gestures, like raising his finger to make a point in discussion. Tendency towards underlining his own importance. Considerable sensitivity of feelings and imagination. He exhibited sensual and imaginational overexcitability (but limited only to things connected with his person) as in touching, or in the religious ritual of his church where he was a leader. Rather weak inner psychic transformation. Lack of internal conflicts, Weak developmental dynamisms. Superficial hierarchy of values, not worked through and weakly realized in his life. To avoid feelings of guilt in his sexual relations with women he protected himself by an elaborate ceremonialism so that he as a superior being descended down to bring happiness to his humble female companions. One can see this in the predominance of formal approach over experiential and emotional, of ritual over internal content. He was very pedantic about his eating habits and also his sexual relations for which he dressed up in a ceremonial manner.
Interpretation:
Definite preponderance of unilevel disintegration. Considerable transmitability of psychical events to the autonomic nervous system evident in the precise timing of his psychic tensions and subsequent functional disorders of his heart and digestive system. Hypochondriacal and neurasthenic tendencies.
These tendencies were increased by his lack of sense of the inappropriateness of his own behavior and absence of any alterocentric inclinations. This resulted in an “escape into sickness,” which lie used as a partial justification of his insufficient responsibility for his own behavior. This in turn caused psychic fixations to specific somatic areas such as the cardio-vascular and the digestive system.
Clinical diagnosis:
Neurastheno-hypochondriac.
Prognosis:
From the viewpoint of positive psychic development—doubtful; strong tendency to primitive integration.
90
Treatment:
M.L. was highly intelligent. The task of therapy would be to show him the inconsistency of his behavior with his intellectual level. It would appear fruitful to evoke some disquietude in ham in relation to his sexual behavior. Namely, the fact that he avoided marriage brought tensions within ham and would disturb him during his beloved rituals. Since his ceremonies and rituals were most important to him he possibly could face, marriage as a means of bringing his life into order. Out of fairness it should be added that there was a woman who wanted to marry him at any cost.
5. Case 9
K.J. was a 41-year-old man, married, an administrative officer in a cultural institution. He suffered—in his opinion—of cardiac neurosis dating from the time of his military service. Lately he often had obsessional thoughts (whether he has made some wrong decision; whether he was acting right; whether he was doing any damage to others; whether he was well thought of). Even for reason of some small impropriety, he excused himself, telephoned, was always excessively apologetic. He was worried about his own “mental unfitness.” He avoided all collisions, had a tendency to exaggerate. At times of strong psychic tension and increasing obsessions he had suicidal thoughts. Nothing brought him joy. When hearing about some mental illness he applied it to himself and either believed to have the same symptoms or expected to develop them in the near future. When his superior said of one of the employees that “he had a black card in his life” he was so upset that he could not sleep. He transferred this “black card” onto his own life, and believed that he was doomed.
There was no evidence of negative hereditary load. Mother was alive. Parents had a good relation, took good care of him. The patient deeply grieved the death of his father.
His marital relationship was good. Both psychical and marital conditions were good. He had one son who posed no problems. During the war he was forcibly re-settled out of the country,
91
had the conviction that he was being followed, and was continuously surrounded by some suspicion. In those days these were frequent but nonetheless painful experiences. Lately he was given tranquillizers and directed to the mental health clinic.
The patient was a capable employee, occupied a managerial position, advanced in his career, was an able organizer. However, he did not like movies or theatre whenever a complicated psychological drama was portrayed.
He came from a culturally deprived background to a culturally rich milieu and rose to some significance in its administration.
General neurological examination:
Pulse accelerated, blood pressure 150/105, red dermographia, reflex responses increased and extended; besides that no characteristic reflex responses. These meager results give more basis to expect that we are dealing here with a sensitivity directed outward (attention to events in his social milieu) with some transfer of his experiencing onto the cardio-vascular system.
Psychological examination:
A mixed type, preponderance of introvert tendencies with rather weak inner psychic transformation (he did, however, sincerely ask me what could he change in himself); some capacity for syntony: obsessions related mainly to external life and without moral aspects. Emotionally responsive. High transferability of psychical experiences onto the autonomic nervous system. Easily affected by suggestion. High intelligence, verbal and abstract as well as practical; symptoms of magical thinking together with some anxiety as to these magical contents (“black card”). Easily yielding to suggestion and thus gets overcome by fears but has no critical power against situations which suggest even a “shade” of danger.
Interpretation:
An intelligent individual of mixed psychological type. His inner psychic milieu is weak. Rising to high level of administra-
92
tive hierarchy with a fair intelligence and a capacity for adjustment and high emotional responsiveness contributed to an excessive sensitivity to public opinion, excessive shyness and care to be “in good order.” This dates back to his traumatic experiences during and after the war when he was questioned by secret police as a result of suspicions and denunciations which in his case were unfounded. The fear of such situations remained which points to a weak inner psychic transformation. He was lacking insight into himself (he avoided movies and books with any degree of psychological depth). With a strong need for adaptation to his environment this formed an attitude of “taboo,” non-involvement, and formally proper behavior. His anxieties, fear of questioning, obsessions of imminent danger, formed sets of symptoms that were “closed,” isolated from the possibility of self-criticism and inner psychic transformation, This was his inner half-conscious “taboo.”
Diagnosis:
Psychasthenia with symptoms of obsessions at a rather primitive level, although approaching the borderline of unilevel and multilevel disintegration.
Prognosis:
Uncertain.
Treatment:
Strengthening and development of general culture, increase and deepening of psychological knowledge of self, slow bringing to awareness and development of the inner psychic milieu. Development of a more independent attitude toward his external environment and towards his social taboos.
We now proceed to a general description of several syndromes from the standpoint of the theory of positive disintegration.
6. Hysteria
The process of disintegration in hysterical neurosis is mani-
93
fested by an increased sensual excitability, by ambivalences which are predominantly affective, by partial suggestion and autosuggestion (not embracing the whole psyche but rather its particular areas), by a tendency towards extremist attitudes, by particular psychomotor reactions (prespasms, functional or hysterical paralysis). Strong affects are always involved.
These reactions are present in Case 5 and in Case 7. In Case 5 we see Irene gradually “sinking” into a state of considerable emotional automatism. Her field of consciousness is narrowed down to her mother and everything that pertains only to her. The end result is dissociation. Her consciousness has split into two persons living separate lives.
Case 7 represents narrow forms of suggestion and auto-suggestion. They are limited to the need of becoming a mother. This is expressed in the somatopsychic symptoms of her conviction that her abdomen was enlarged.
Considerable suggestibility so characteristic in hysteria indicates a weakness of the inhibiting power of higher psychic centers. This suggestibility is on a fairly low level because it yields to trivial thoughts and perseverations without much content, especially as in Case 2.
In a great many cases of hysterical neurosis we observe partial symptoms often occurring consecutively. For example the little girl mentioned on page 75 developed the symptoms, as her father did, in a series of increasing seriousness. She developed partially one after another immobilization, sleepiness and finally a hysterical paralysis as an unconscious imitation of the same sequence of her father’s actual physical illness.
7. Neurasthenia
Neurasthenia was considered by Pavlov to be not a purely human neurosis but one especially common among laboratory animals. In my view, it is a psychoneurosis exhibiting a basic mechanism of disintegration. We observe in it cyclic states of excitation, stimulation and arrest of psychic functioning shown by states of fatigue or exhaustion. The cyclic pattern of excitation and inhibition, already emphasized by Pavlov, is a characteristic indicator of a disintegrative process, since it upsets
94
the homeostasis of an established rigid pattern of behavior. The characteristic for neurasthenics periodic creativity and easily following fatigue, may indicate that the disposing and directing center is not sufficiently strong either in the area of drives or in one of the higher psychic functions. Considerable fluctuation of moods and disturbances in sexual functioning also reveal the presence of processes of disintegration. A neurasthenic has an inferiority feeling because of the weakness of his drives, as well as because of a disequilibrium in his sexual life and his incapacity for systematic mental work which usually demands considerable tension.
A strict distinction between neurasthenia and psychasthenia may not be necessary. We are inclined to regard neurasthenia as a lower level of psychasthenia. One can say that in neurasthenia neuropsychic processes are more active (autonomic dystonia, at times strong pressure of basic drives with their simultaneous inhibition visible, for instance, in a strong sexual excitability combined with shyness and anxieties such as fear of impotence, fear of venereal disease, etc.), while in psychasthenia mental processes are predominant.
Psychasthenia is a “self -sufficient” syndrome. It operates on the terrain of higher development with a clearly active disposing and directing center. It is much more independent from the stimuli of the autonomic nervous system and from the pressure of strong biological drives. This is easily seen in S.M. (Case 6) whose experiencing, and thus his psychoneurotic processes, take place on a very high level of altruistic feelings, moral concerns, and transcendental obsessions.
Other processes and a lower level of symptoms in the same “psychoneurotic family” are present in Case 8, where we observe psychosomatic symptoms, especially in the cardiovascular and circulatory systems, plus the dependence on ritual, on showing oneself off. There is thus a distinct dependence on external opinion, characteristic of lower levels of psychoneurotic processes.
The difference between neurasthenia and psychasthenia, or as we would rather say, between the lower and higher levels of psychasthenia, is also evident in the need for different therapeutic
95
methods. Since in psychasthenia the psychic processes are dominant, therefore, the most effective method is autopsychotherapy and therapy promoting individual growth through educative methods; in neurasthenia results may often be obtained more readily with drugs such as antidepressants, tranquillizers and others which regulate the disharmony between the autonomic systems. Depending on the level of development of emotional functions in cases on the borderline of neurasthenia and psychasthenia one applies mainly either appropriate pharmacological drugs or methods leading to autopsychotherapy (such as educative or even “philosophical” therapies).
8. Psychasthenia
Psychasthenia is characterized by phobic symptoms, obsessions and anxiety, but especially fears, obsessions and depressions of the existential type.
Psychasthenics have a weak reality function at the low level and weak basic drives. They often have a high level of analytical reasoning but periodical weakness of synthesis.
An ability for global synthesis, for retrospection and projection into the future (as discerning one’s own direction of development, definition of aims in terms of changes in one’s personality structure), delayed responses yet great intelligence and weakness of primitive functions are phenomena in evidence of certain splitting into levels. We have already mentioned the “self-sufficiency” of many psychasthenics—their self-confidence and activity in their own inner psychic milieu. Perceptions, ideas, memory stimuli—all this can develop and reach greater complexity without the participation, or with only a minor one, of the external milieu. The woman in Case 2 did not care at all what others were going to think of her, whether her material needs were going to be satisfied or not, or when she was going to die. Her interests and her experiencing were focused on her own essences. This picture clearly demonstrates multilevel disintegration, loosening and—in some cases—extinction of primitive drive integration.
As a rule the development of higher functions disorganizes
96
lower functions before a new and higher organization can be established. Primitive drive structures which unite into a whole the basic drives and those of intellect and emotional life, undergo definite loosening and disorganization. There results in inability for integrated action. Mental functions in a loosened structure: no longer serve the primitive impulses of a low structure. Those functions now are somewhat independent, forming “fixations” to various loosened drive complexes, which are usually in conflict with each other. Emotional activity is no longer organized into a coherent whole, and is no longer guided by the pleasure principle and the avoidance of pain.
The arrest or inhibition of such activities as social events, ordinary preoccupations, intrigues, professional ambitions causes helplessness, uncertainty in decisions, weak activity at the abandoned level of reality. The reality which a psychasthenic partially reaches at a higher level is often strongly held, but insufficiently controlled; hence, the uneasy state of “suspension” arises as a result of having left one level and not having yet reached the new level. One of my patients described it in these terms: “I am between heaven and earth. I am tormented by not belonging to either one. What one does on one level I am no more capable of, what one does on the other I haven’t yet learned.”
There is then “disquietude” and disharmony on both levels, but in particular anxieties arising in relation to being conscious of the alien nature of the frequently recurring stimuli from the lower levels. This also causes astonishment. In the case of Korczak’s psychoneurosis there were tensions, shock and crises in the free of the brutal realities of life which he had to struggle against in order to provide for the children in his school in the ghetto. Korczak in his personal life also experienced inner tensions in relation to his occasional heavy drinking when he was incapable of controlling his own moral anxieties and scruples. In the case of Unamuno, who with great dedication tried to counteract the ‘evil' rampant in his scientific and social milieu, the collision with the alien stimuli from lower levels caused him extremely painful shocks.
97
Uncoordinated movements, timidity, and excessive inhibition lead to loss of security in daily life. Claustrophobia, fear of heights, fear of space, of new situations indicate a lack of equilibrium between one disposing and directing center and another one not yet fully formed at a higher level. These reactions are again an expression of fears resulting from the state of “suspension.” The individual is afraid of isolation and at the same time of an open space. It is a fear of “closed” attitudes and of “open” attitudes, of a road leading forward and of a road leading back.
A similar situation is observed in a disequilibrium between the introversion and extraversion tendencies (anxiety and internal feelings of uncertainty). The pattern of introversion and extraversion is disturbed in psychasthenia by dynamisms of transformation which now press for some degree of liberation from purely biological control and from behavior after only one type of pattern. The states of anxiety and obsessions frequently go together with this state of “suspension” between levels which necessarily is a state lacking in psychical stability. [see also Chapter 7, Section 3 (1)].
Obsession and anxiety psychoneuroses are thus often persistently associated with psychasthenia (Dąbrowski, 1967).
9. Psychoneurotic depression
Psychoneurotic depression is characterized by a great tension of sensitivity and by a strong fear of being psychically hurt. Hence withdrawal, isolation, feelings of inferiority, fatigue, fear of activity and periods of low mental tension (low energy) alternating with periods of high emotional tension. We also observe weakening of ability for synthesis but intensification of analytic tendencies.
When the developmental potential is considerable then depressions are usually of internal origin, i.e. arising spontaneously within the individual himself. They are the expression of his disquietude with himself, feelings of inferiority in respect to himself, dissatisfaction with himself, feeling of guilt. It is a consciously or half consciously experienced distance between
98
himself from the “higher level” that he sees and feels to exist within him, and himself from the “lower level” that he also sees, evaluates negatively, and observes in its weakness, misery, humiliation and worthlessness. One of my patients expressed it in the following words: “I am surprised that my children can love and care for someone so unpleasant and repulsive as myself.”
Depressions, as a rule, develop on the matrix of inner transformations with a more or less pronounced influence of the external milieu. Very often they are related to the psychobiological changes of maturation and the climacteric. In both these periods something new arises and something ends. In the period of maturation the new may be incomprehensible, strange even unpleasant, and that which ends causes sadness. Then come thoughts of death, suicidal inclination, and—not infrequently—suicide itself. This period is followed fairly often by development and unfoldment of mental energy and positive traits.
The climacteric has certain similarities, although from the biological aspect, the phenomena are not only new but also difficult and unpleasant because there is a diminution of energy, of efficiency, loss of beauty, and awareness of somatic discomforts. In the experiencing of an individual aware of himself there is a feeling of losing one’s attractiveness, one’s value and instead growing dependence on others. Individuals endowed with great developmental potential experience suicidal thoughts, preparations for death, and often changes in the direction of opening interest in meditation and mystical phenomena. At the same time they are dominated by feelings of sadness, isolation and loneliness.
10. Psychoneurotic Infantilism
Psychoneurotic infantilism is manifested by enhanced excitability of affect and imagination, by timidity, extreme enthusiasm, great richness of fantasy and new ideas, inhibitions, disappointments and depressions, traumas as a consequence of a weak reality function. These characteristics place psychoneurotic in-
99
fantilism closer to psychasthenia than to hysteria. Hence “collisions” in daily life; hence a weakening of reality function at a low level; hence a tendency for regression among adults as well as among children.
By regression we mean a return to early stages of development. It provides a strengthening of prophylactic and protective forces against too strong shocks of everyday life, hence, also, the so-called “positive regression,” as an expression of a desire to be surrounded with an atmosphere of affection, sincerity, and freedom from inappropriate forms of adjustment. Psychoneurotic processes make individuals more sensitive. This tender stage of development requires protection—“positive regression” serves here as a buffer.
11. Sexual Psychoneurosis
In sexual psychoneuroses we usually encounter sensual excitability as a part of a wide area of psychic hyper-sensitivity, together with symptoms of sexual inhibition and anxiety (e.g. elements of neurotic fetishism and necrophilia); hence excessive sexual idealization, and sexual attraction to more mature persons.
It is important to distinguish syndromes of sexual psychoneurosis from those of sexual psychopathy; the latter are expressed by normal or perverted sexual drives which are so strong that they give a dominant character to behavior and personality.
Psychopathy is an integrated structure of primitive drives. It is a structure dominated by constitutional control, lacking in self-awareness and therefore representing a low level of development. The psychopath lacks syntony with others, there is no trace of empathy, and he has no inner conflicts. The motivating forces of behavior are basic needs stemming from basic drives. If such an individual has in his psychological make-up a strong sexual excitability then this will express itself in a primitive form of aggressiveness or sadism.
In contrast to psychopaths sexual psychoneurotics have complicated sexual tendencies beset by inhibitions, phobias, masturbation, homosexuality, idealizations and strong inner conflicts
100
in regard to their sexuality. In this respect one should differentiate, as in the case of other psychoneuroses, different levels of homosexuality in order to distinguish its psychoneurotic processes (on a higher or even very high level) from processes closer to psychopathy occurring much less frequently.
12. Psychosomatic disorders
One of the underlying causes of psychoneuroses of organs and of systems of organs is an excessive ability to transpose emotional experience onto the autonomic nervous system. In the psychoneurotic process there is either domination of the dynamisms of the psyche or of the somatic dynamisms of the autonomic nervous system. This domination may last for a period of time or be established for good. It depends on the power of the developmental potential and on the evolution of the collisions with the external milieu and on those occurring within the inner psychic milieu.
When mental dynamisms predominate then the psychoneurotic process “upgrades” its level. When the dynamisms of the autonomic nervous system predominate then we observe characteristic for this system disorders and the mental dynamisms (which always involve a certain degree of self-awareness) play only a marginal role. In consequence the neuroses of organs and their functions are chronic. We observe frequently unconscious (or very weakly conscious) tendencies to combine a diffuse psychic excitability, particularly sensual and psychomotor, with those organs or their systems which can show marked disturbance of function. We see then disorders involving the digestive system, the heart or the cardiovascular system. The psychical processes are thus superimposed on the disorders of physiological functions. Emotional difficulties become fixated to certain organic functions. Although this creates further complications, it nevertheless brings relief to the patient by localizing his overall excitability in a more or less recognizable territory.
In psychosomatic disorders we usually deal with a very strong inner tension and with an insufficient transformation ability. In order to be able to carry out a positive transformation of
101
emotional difficulties one has to have a more or less clearly developed hierarchy. There have to be at least some initial elements of the dynamism “subject-object in oneself”; there has to exist the differentiation between that which transforms and that which is to be transformed.
This ability is lacking in the process of unilevel disintegration. Strong inner conflicts and strong external “collisions” create such tensions that a person is in no position to work out their transformation but is forced to seek at first palliative actions, which may take the form of hyperkineses, tics, unconsciously controlled spasms, etc. The lack or insufficiency of inner psychic transformation makes psychosomatic disorders a common phenomenon in unilevel disintegration and the beginning of multilevel disintegration.
102
CHAPTER VII
INNER PSYCHIC MILIEU IN PSYCHONEUROSES
1. Origin and Development of the Inner Psychic Milieu (1)
(1) Unilevel disintegration.
A lack of balance between the sympathetic and the parasympathetic nervous systems (so-called autonomic dystonia) can be regarded as an unconscious or semiconscious nucleus of an inner psychic milieu. The individual experiences a disturbance of his internal feeling. He becomes aware of some internal “noise” in his organism. His sense of well-being is disturbed, his sleep or his digestion are out of order, he may tire more easily than before and to all appearances for no apparent reason. These irregularities and perhaps some pain and fear associated with them, begin to direct his attention inwards.
The merely psychophysiological aspect (i.e. where there is little awareness and little conscious experiencing of mental and emotional processes) is characteristic of psychosomatic disorders. They mark—in the domain of drives and emotions—the collision of various subconscious unsystematized forces as “something is happening in the inner milieu.” There appear excessive tensions, conflicts between various tendencies, ambivalent attitudes, conditions of excitement and depression, easy yielding to suggestion or autosuggestion, symptoms of conversion. In all this consciousness is not much active, there is limited, if any, psychic localization or hierarchy, that is to say, there is limited, if
___
(1)The structure and dynamisms of the inner psychic milieu are described in detail in “Mental Growth” (Dąbrowski, Kawczak, and Piechowski, 1970).
103
any, conscious organization. These phenomena and internal sensations occur as if on one plane only; there are no inner conflicts between the consciousness of the “higher” and the “lower.” There is only one level of activity. We observe this in most psychosomatic disorders such as hypochondria, neurasthenia, lower levels of hysteria, etc., as in cases 4, 7 and 8.
This fact, repeatedly observed, led to the hypothesis that psychosomatic disorders such as neuroses of organs and of systems of organs are more frequent at the stage of unilevel disintegration and the stages overlapping its borderlines. We observe here somatic fixations and localization of psychological difficulties because higher psychical centers are too weak in their transforming power. The dynamic factors of multilevel disintegration are not prominent, and are rather weakly developed. Such dynamisms as astonishment with respect to oneself and disquietude or dissatisfaction with oneself appear only vaguely or sporadically. There appears a variety of disposing and directing centers, as in cases 5, 7, or 8, since an autonomous disposing and directing center operating on a higher level is not yet developed. (Such center functions hierarchically, i.e. it controls and harmonizes lower levels of activity). Instead various divergent tendencies or impulsions act in turn as disposing and directing centers. In case 5 these were: Irene’s desire to bring her dead mother to life and on the other side the acknowledgement of her death to which Irene reacted with a catatonic withdrawal. The nuclei of the third factor, or the awakening of the inner self, were still weak, only rather ambivalently or intuitively anticipated.
(2) Multilevel disintegration: spontaneous vs. organized.
As multilevel disintegration assumes importance, we observe an increase of positive (i.e. developmental or directional) elements in psychoneurosis. The inner milieu is being gradually formed into a hierarchical structure by passing through a somewhat subconscious stage in the first phase of multilevel disintegration, wherein new dynamisms are being “born,” such as astonishment towards oneself, disquietude, dissatisfaction with oneself, feelings of inferiority and guilt.
104
As the development continues on, the individual comes gradually to an elaboration of his previous experiences. There is now a significant degree of tranquility and harmony in his inner psychic milieu. Now it is the individual himself who takes the initiative in organizing a hierarchy of his own inner contents, while in the preceding stage of development it was the contents and the experiences themselves that were pressing for change and growth (hence the name of the previous stage “spontaneous multilevel disintegration”). This is now the next stage of multilevel disintegration, the stage of organization of disintegrative forces, the phase of transformation, whose characteristics are such dynamisms as “subject-object in oneself,” the “third factor,” the awareness of control and of one’s own inner psychic transformation in the direction of changing one’s psychological type, and even the biological cycle of human life (Dąbrowski, Kawczak, and Piechowski, 1970).
With a continuing progress of development we observe the approach of secondary integration signaled among others, by such dynamisms as a strong disposing and directing center at a higher level, personality ideal, dynamism of autonomy and authentism, responsibility.
(3) The level of psychoneurotic disorders as a function of the developmental level of the inner psychic milieu.
Comparing the three stages of positive disintegration, i.e. unilevel, spontaneous multilevel and organized multilevel, we can say the following. These three stages are also the three different stages in the evolution of the inner psychic milieu. Unilevel disintegration is characterized by psychoneurotic syndromes that are scarcely conscious, ahierarchical, that have a jumble of symptoms like ambivalences and ambitendencies; hence depressions, anxieties, obsessions, and psychosomatic disorders of stereotype closed character, without discernible channeling towards further development. In consequence the disorders are usually grave and the prognosis not always positive.
The apparent equivalence of many different directions, the wide range and seriousness of mental disorders influence many
105
patients to distortions in their perception of reality. It is a consequence of a total lack of internal organization and of any directionality in their disorders. The unilevelness and distinct pathology of this stage of development is reflected in the creative output of many authors who have not gone beyond this stage. Their creativity is “value-free,” i.e. lacking the sense of a hierarchy of values, it depicts reality as degenerate, stagnant, cynical, with “no exit.” This applies to the lower levels of existentialism.
The transition to the next stage is characterized by the appearance of a new factor, whose significance for development cannot be overestimated. This factor is a channeling upward which now becomes active. This is the dynamic factor of a hierarchization of values (cf. p. 39). This stage is dramatic, sometimes tragic, marked by sharp turning toward oneself in order to seek solutions within oneself. Grave intrapsychic conflicts like doubting one’s own worth, doubting the meaning and the sense of life, facing one’s own responsibility, are met with the dynamism of inner psychic transformation which directs them “upwards.” The state of hopelessness lifts gradually.
The subsequent stage of organized multilevel disintegration is a stage of recognition and classification of difficulties, taking them into one’s own hands and incorporating them into a development leading toward a clearly perceived personality ideal.
The higher the development of disintegration the stronger is the role of integrating forces. The progress to higher levels of disintegration can be seen in different characteristics of psychoneurotic symptoms and syndromes where there is an increasingly stronger accent on the consciousness of internal conflicts, depressions, anxieties and obsessions of increasingly more existential and altruistic nature, and with an increasingly better defined level of self-awareness and self-control. The lower dynamisms of the inner psychic milieu submit through self-awareness, self-control, activation of the ideal, empathy to the transforming activity of creative forces, of the forces of self-perfection and secondary integration. Each of those dynamisms is being considered and used from a number of viewpoints, and
106
at various levels. In each of them one can see its developmental history, starting with automatic development, a period of loosening up, the passage from an unconscious stage to a positive, fully conscious, creative level. In the progress of development of each one of these dynamisms one observes the separation of lower, more automatic, less conscious and less defined levels from more autonomous, more conscious, more complex, more altruistic, and more clearly defined higher levels. This concerns such dynamisms as astonishment with regard to oneself, feelings of guilt, inner psychic transformation and other.
The inner milieu ceases to be a collection of psychic functions, becoming rather a versatile, organized and hierarchical instrument of the developing personality and its ideal.
The analysis of the levels of development, and therefore, of the levels of the inner psychic milieu, in relation to both healthy and pathological dynamisms gives us a differentiating tool that can be applied to psychoneuroses. Thus we distinguish different levels of psychoneuroses related to different levels of development, for instance, hypochondria is characteristic for unilevel disintegration (level II), and psychasthenia is characteristic for advanced spontaneous multilevel disintegration (advanced level III); neuroses of organs characterize unilevel disintegration, while psychoneurotic depressions of the existential type characterize spontaneous multilevel disintegration (level III) or even borderline of the organized multilevel disintegration (level IV).
We differentiate also levels of the same psychoneurosis (intraneurotic levels), for instance, the lowest level of hysteria (borderline of level I and II) is a characteropathic hysteria, while at level II and borderline of level III it is conversion hysteria, and in the transition stage from level III to IV it is a hysteria of existential character marked by a deep empathy toward others, with dramatic attitudes, and even elements of meditation and ecstasy (See Table II and its legend).
2. Inter- and Intra-Neurotic Hierarchies of Mental Structures and Functions
Evolution, according to Jacksonian and neo-Jacksonian con-
107
cepts, consists of a transition from that which is simple to that which is more complete, from that which is better organized to that which is less organized, from the automatic to the deliberate (Jackson 1958); Ey and Rouart, 1938).
Involution consists, then, of a process in which the above order is reversed.
According to both Jackson and the neo-Jacksonian school, neurotic symptoms are an initial stage of mental involution; mental illness is first expressed by neurotic or psychoneurotic symptoms, which increase as the illness develops, causing even deeper disorders and eventually the dissolution of psychic functions.
The theory of positive disintegration (Dąbrowski, 1964a, b) represents a diametrically opposite view. According to this theory psychoneurotic symptoms, except for a rather insignificant percentage gravitating towards involution, are expressive of positive human development. One could almost risk a statement that creative human development is rarely, if at all, possible without some nervous, neurotic, or psychoneurotic dynamisms.
Personal development usually begins with increased psychic sensitivity and with more or less hidden psychoneurotic processes; and so, contrary to Jackson, various forms of nervousness and psychoneurosis mark positive psychic development, rather than the spreading of mental illness. The best supporting material for this is the study of biographies of eminent individuals (see Chapter 10).
The rudiments of talents which are inherited and manifest themselves early are usually clear indicators of development through spontaneous multilevel disintegration and associated psychoneurotic symptoms. Nuclei of internal conflicts also point to this character of the developmental process and related to it psychoneurotic processes. Early manifested self-control combined with positive maladjustment allows one to foresee an even more advanced level of development (organized multilevel disintegration) and to postulate the future appearance of depressions, existential anxieties and obsessions.
The stimulus directing the early development of
108
self-control is in most cases the combined activity of astonishment with oneself with the dynamism of growing awareness. This can be observed in small children—when they react to particular conflicts with their environment, as for instance when the child is worried because he received undeserved praise and at the same time is present to his innocent friend being blamed for something. An attempt to console his friend in such a case is not only a sign of a child’s sympathy but also of self-control. If a sensitive child shows greed for some food and is driven to reach for bigger and better morsels one can also observe that such greed is tempered fairly quickly by his noticing that his sibling or his company will get less.
Depending on the kind and degree of genetic endowment—which provides the nuclei for personality growth—we shall have various levels of psychoneurotic symptoms within a single concrete neurosis or a variety of psychoneurotic complexes different from each other at a number of functional levels.
We could say that an individual acquires such psychoneuroses, as are warranted by his natural endowment and level of development (Dąbrowski, 1964a, b).
Let us try to express our viewpoint in more simple terms. All psychoneuroses can be arranged into a hierarchical system on the basis of their developmental advancement and degree of complication as well as on the degree of separation from the primitive structures and functions of basic drives. From this point of view, the hierarchy, in descending order, could be presented as follows; psychasthenia, psychoneurotic depression, psychoneurotic anxiety, psychoneurotic obsession, psychoneurotic infantilism, conversion hysteria, neurasthenia, sexual neurosis, hypochondria, and organ neurosis. This, of course, is still only an initial attempt at systematization, nevertheless, based on broad clinical experience.
This hierarchy of different psychoneuroses is an inter -neurotic hierarchy. It must be supplemented by an intra -neurotic hierarchy of functions. This is a hierarchy of functions based on. the same criteria as above (self-awareness, degree of self-control, empathy and other mental functions in higher and lower forms), but with
109

110
respect to one and the same “pathological unit,” that is to say with respect to a single psychoneurosis or psychosis. Using these criteria we can, depending on the developmental level of an individual and his symptoms in a variety of psychoneurotic functions, distinguish between several levels in each psychoneurosis (Dąbrowski, 1966; Dąbrowski and Piechowski, 1969).
_____________________
Legend to Table II
This table lists a number of psychoneurotic and psychotic syndromes in the order of their appearance at different levels of development.
Developmental Level I is called primitive or primary integration. This stage is exempt from disintegration and its characteristic feature is that behavior is controlled chiefly by constitutional factors. A primitively integrated individual spends his life in the pursuit of satisfying his basic needs. He is controlled by the integrated structure of his instincts, and his intelligence is in their service. He responds to social influence only as a measure of self-preservation. There are no internal conflicts. Mental disorders are characterized by lack of response to social influence, i.e. other individuals are perceived and used as objects.
Developmental Level II is called unilevel disintegration. At this stage of development psychological factors and social influence enter into play acting largely in an unconscious manner. The previously primitively integrated instinctual structure undergoes a disintegration. Because of limited self-awareness individuals on this level of development transpose their emotional and mental difficulties onto their body via the autonomic nervous system. Hence psychosomatic disorders are a distinctive feature of the mental disorders of Level II. Internal conflicts exist but are usually externalized. They lack a direction, they occur as if on one plane only (hence called unilevel), and for this reason this is also the stage of the most severe mental disorders. The states experienced by the individual are projected outward onto the environment. This process serves as a justification of his behavior.
111
Developmental Level III is called spontaneous multilevel disintegration. It is characterized by a greater degree of conscious involvement of the individual in his emotional and mental life. This fact generates an internal conflict which is an experience of a struggle for mental control between the “lower” and the “higher” within oneself. This is a multilevel conflict which carries the potential for a direction and further development (from the “lower” to the “higher,” i.e. from less autonomous to more autonomous). The experiences and associated conflicts for the most part are brought onto the individual by events in his life. Hence the name “spontaneous multilevel disintegration.” The mental disorders on Level III are characterized by prevalence of psychoneurotic over psychotic processes.
Developmental Level IV: organized multilevel disintegration, Growing self-awareness brings as a result the development of conscious self-control applied in the service of individual growth. This stage of development is characterized by lesser tension and greater ability to systematize experiences and to take the development into one’s own hands. One could say that now in its general outline it becomes independent of the events in one’s own life. Hence autonomy and authenticity. Mental disorders on this level are very mild and arise from intense experiencing of existential and transcendental realities.
A number of syndromes occur on more than one level of development. If the level is low then biological functions control the mental ones and the awareness is limited. The expression of a syndrome is either psychosomatic, or self-centered, or both. If the level is high then mental functions are predominant and the expression of a syndrome loses its psychosomatic counter-part but gains in the intensity and awareness of an inner conflict, and has alterocentric components.
_____________________
The cases presented so far and the Tables II and III demonstrate the intraneurotic differences which we shall now proceed to analyze.
Case 6 is an example of the highest level of psychic structures and functions in psychasthenia which is expressed through obsessions concerning problems of all mankind. This
112

patient shows a very high level of empathy and of responsibility for others. He dwells on a high level of reality rather well
systematized and elaborated. Thus his reality function has developed to a high level and embraces a wide range of ethical and humanistic questions. All the life problems of “others” concern him very deeply, but what is of great significance is the fact that he is moving from experiencing to attempts to make himself ready to actually help others. His existential attitude is thus combined with an attitude of masking his beliefs a living reality.
Case 2 is an instance of psychasthenia on a high level but with an expression of restlessness, drama and crisis. Reality function appears highly developed but of distinctly egocentric character with altruistic inclusions although more theoretical than practical. The tension was directed to herself with a feeling of necessity to bring herself to a distinctly pathological condition or even destroying herself. This is an attitude of antinomy between the need to either achieve the highest level or to destroy oneself.
113
Case 9 represents psychasthenia on a much lower level and in fact near to neurasthenia. K. J. shows an ambivalent attitude of being alterocentric and egocentric. He feels close to his family, but in a highly egocentric even magical way is geared to his environment. He shows fears of himself in the sense that he is afraid he will do something improper that would have detrimental consequences for himself and his family. His reactions and attitudes show thus a weakness of his inner psychic milieu. His neurasthenia is related to obsessive and anxiety states stemming from his care to avoid conflict with his environment. There are strong unconscious components (the “black card”) which—to a large extent—are responsible for considerable tension.
Case 8 represents the lowest form of psychasthenia with symptoms of hypochondria, neurosis of organs and rather narrow egocentrism. His mental effort to control his feelings of inferiority, disquietude, hypochondria is carried out by means of magical actions—ceremonialism which externally elevates his sense of self-worth.
A different “psychoneurotic family” is represented by cases 5 and 7 which are examples of two different levels of hysteria. Case 5 (Irene) is a manifestation of empathy narrowed down to Irene’s mother, nevertheless an empathy on the highest level. There is in it a strong feeling of responsibility for her, an extraordinary capacity for self-sacrifice, endurance of privations and lack of sleep. The death of her mother as a shock of unbearable stress split Irene into two persons separated from each other by a complete change of the frame of her consciousness, this is a case of somnambulism where this split of personality is most likely a preventive measure that saved Irene from suicide or severe schizophrenia.
Case 7 is very clearly an example of a fairly low level of hysteria. There is in it a marked degree of suggestibility and autosuggestibility directed primarily by selfish motivations. There is magical thinking in the service of primitive drives, and likewise with the symptoms of conversion.
In the “family” of obsessions and anxieties Case 3 represents
114
a very high level. We note in this young priest moral refinement and sensibility, feelings of responsibility for others, feelings of sin and guilt without any clearly demonstrable transgression on his part. We observe in him a process of hierarchization and an authentic attitude towards his ideal.
Case 4, on the other hand, is an example of a low level of psychoneurotic anxiety, where the fears and obsessions concern only external events. There is no inner psychic transformation, instead strong manifestation of concern with survival (low level of the self-preservation instinct), obsessions with magical contents (repeating numbers, avoiding situations that brought her “bad luck”). These reactions are not subject to attempts to control and alter them by reasoning that the situations that brought them about are part of life and happen to others too. There is also no attempt to step outside of her egocentric sensations which are more related to her body than to an awareness of herself as a person. That is why we can say that there are no signs of inner psychic transformation.
3. Levels of Functions in Psychoneurotic Syndromes
We have discussed earlier interneurotic differences in the levels of functions. Table II makes this clear. The levels of development (I—primitive integration, II—unilevel disintegration, III—spontaneous multilevel disintegration, IV—organized multilevel disintegration) have characteristic syndromes of mental disorders. As an example we can point out that psychasthenia on a high or medium level, or anxiety psychoneurosis on a high or medium level represent much higher forms of developmental functions than neuroses of organs, sexual neuroses or such forms of psychasthenia as neurasthenia or hypochondria.
Characteristic psychoneuroses of unilevel and multilevel disintegration are: psychasthenia, psychoneurotic obsession, psycho neurotic anxiety, depression and psychoneurotic infantilism.
We now proceed to a general description of different levels of these psychoneurotic syndromes.
115
(1) Psychasthenia
As its name indicates psychasthenia (psychic asthenia) is a result of a weakening of mental functioning. We have to find out what functions appear to be weaker. In the conception of the theory of positive disintegration an analysis of mental functions becomes meaningful if one introduces the differentiation of levels of functions. Applying this to psychasthenia we shall discover that some levels of psychic functions are attenuated or diminished while other ones are strong and well developed. One of the functions representing in psychasthenia a higher level is the reality function. It is a function organizing the mental life of a given individual. Individuals “suffering” from psychasthenia in its higher form display weaknesses and deficiencies in handling the affairs of their ordinary living and its burdens but tend to function well at higher levels of reality. Their reality function is thus weak on a low level but well developed on superior or high level. Such individuals may be creative with enhanced excitability of imagination and affect, with high empathy, with an ability for synthesis, for organizing and carrying out their work on a high level. The synthesis on a higher level is not possible under the dominance of everyday reality. This is why it is necessary to break away from it.
Such individuals have deficiencies in their adjustment to lower levels of reality. The action of the “third factor” (the mental factor of conscious discrimination in one’s development) and of the dynamism “subject-object in oneself” is usually very good, but still failing to encompass the whole personality structure. However, the lack of sufficient adjustment to ordinary reality causes it to be pushed aside and neglected without being understood. Hence disquietude and dissatisfaction with oneself in relation to this level of reality, hence attempts to escape from it, although such escapes are not well thought out. However the lower level is not a source of strong anxiety. This means that the individual feels that he belongs more strongly to the higher level than to the lower one. For this reason the disquietude and the dissatisfaction with the activities on lower level is not very strong.
116
The consequence of this dichotomy is an ability for inner psychic transformation on a medium and high level and at the same time considerable difficulty in transforming the lower levels of functions. Instead of being transformed these lower levels are suppressed and pushed aside. The psychasthenic, therefore, moves away from the lower level of reality because he has more creative power and potential for growth at a higher level. Thus his inner psychic transformation is also greater at the higher level. In the moral sphere, for example, this denotes moving towards realizing what “ought to be” and moving away from “what is.”
Obsessions frequently occur together with psychasthenia and usually originate in the higher level. They express moral attitudes and sophisticated existential contents. On this level of psychasthenia obsessions are the result of a desire to reach a higher level.
On a lower level of psychasthenic syndromes there is no hierarchization or a weak one, there is no separation of the reality function on a high level from its operation on a low level. There are aspirations, tendencies and thrusts toward higher level of development but at the same time there is an attraction and partial adjustment to the lower level. In consequence of this vagueness or even lack of developmental direction there are tensions and depressions, isolations from everyday life and interchangeably an attraction to and moving away from higher levels (ambivalences and ambitendencies), lack of sense of security. This hesitation and lack of orientation causes states of considerable tension. These fluctuations between levels, the projections in both directions of reality (high and low) causes something like a state of suspension. Related to this state are periods of unbearable feelings, tendencies toward autism, even suicide. If the individual will not firmly root himself on a higher level of his reality function he will be exposed to pulls from both the lower and the higher levels.
As we move lower in the hierarchy of psychasthenic complexes we shall find greater similarity to neurasthenia.
A lack of hierarchizing dynamisms, and hence a lack of
117
broader perspective and capacity for synthesis localizes the tension on a lower level in the form of somatic fixations. This is one of the causes of the neuroses of organs. This lower level is then frequently beset by neurasthenic syndromes expressed as tensions, fatigue, feelings of not being able to cope, disorders in the functions of organs, and considerable egocentrism.
In the extreme case of tensions without visible developmental possibilities we encounter a process of considerable narrowing down of mental activities to the disorders of the autonomic: nervous system, to the disorders in the functioning of different organs, to the disturbance of inner feelings, to a constant feeling of discomfort expressed in different forms of hypochondria.
Especially characteristic here will be a weakening of creative tendencies, considerable tendency towards both physical and mental fatigue, generally global feelings of inferiority without any compensating factors in creativity, hypochondriacal tendencies, disorders of sexual functions.
It is to be understood that the higher the level of function, the stronger its connection with the process of multilevel disintegration, while the lower the level, the more it is related to the process of unilevel disintegration. Different levels of psychasthenia are exemplified by Case 6 (the highest level), Case 2 (high level) and Case 8 (low level—neurastheno-hypochondriac).
(2) Psychoneurotic Obsession
This is the most complicated and the most difficult to deal with type of psychoneurosis. Here we shall discuss only very briefly the problem of intra-neurotic functions in psychoneurotic obsession. Psychoneurotic obsessions are treated more fully in Chapter 8.
When obsessions stem from the highest psychic functions and the most outstanding traits of man then we have the highest level of obsession. They can be said to be normal for an individual on a high level of development. These are, for example, obsessions of heroism and self-sacrifice, obsessions of responsibility and love, or obsessions of existential character involving
118
empathic tension in response to the suffering of others and actual readiness to help them.
Already on the third level of development (spontaneous multilevel disintegration) with its dramatic sequence and strong internal conflicts obsessive elements can frequently be found in astonishment and disquietude with oneself. We may observe, for instance disquietude with oneself of such tension that it causes insomnia. In the feeling of guilt and sin there are often very strong obsessive elements of a high degree of tension and covering a wide field of experience. This fact explains why the disposing and directing center, the third factor and dynamisms of control, in spite of their considerable power yield sometimes to obsessional tendencies. Inner psychic transformation progresses then only with much difficulty.
On the lower level of psychoneurotic obsessions we find such unconscious or half-conscious obsessive symptoms as tics, phobias, obsessions of a magical and ceremonial character (e.g. obsessive washing of hands), and so on.
These levels of obsession psychoneuroses are demonstrated in Case 3 (high level) and Case 4 (low—unconscious level).
(3) Psychoneurotic anxiety
We find in anxieties many intraneurotic levels of functions. On the highest level we encounter anxieties of existential character concerning one’s family and friends, anxieties about people who suffer, who are exposed to injustice, who are humiliated, anxieties for all those who will suffer in the future and who will be victims of fate. Frequently such anxieties are related to a strong pressure of the feeling of responsibility. At the same time they often reach out to all people and all living creatures and, in a way, become cosmic anxieties. Such anxieties appear in people of high moral development, great empathy, who are capable of identifying with others.
Psychoneurotic anxieties show symptoms similar to psychoneurotic obsessions with the difference that the third factor and the disposing and directing center assume a more prominent
119
developmental influence. Clinical observations show that when the level of individual development is high then psychoneurotic anxieties allow a much stronger activity of these two dynamisms than in the case of psychoneurotic obsessions which engage the psyche too strongly in pathological complexes.
At a high level of psychoneurotic anxiety the intellectual component of anxiety experiences is usually rather high. We also find that the individual realizes the motivational value of his anxiety states. In an anxiety of the existential type, related to a sense of r responsibility for moral issues, we find fear of yielding before necessities, before anonymous or mysterious phenomena, with a strong projection of programs of escape from the insupportable tension of those anxieties, alternating with recoil from such programs. The individual feels open and “invaded” by the anxieties experienced by others, as if by a “cosmic” anxiety. His sense of responsibility is not based on a contract but on a universal sensibility. It is like an embodiment of “come ye all to me”; he feels wounded by the dread in the lives of other people. Dr. Korczak is an example: in order to save the children in his school from the terror of death in the crematorium he told them they were going on a picnic. He stayed with them to the last. In this way by sacrificing himself he stopped the fear of death from reaching the children.
At a lower level we shall find anxieties of a less general character: anxieties fixated to some specific areas connected with ambivalence of feelings and tendencies. Here we observe anxieties about the welfare of the family, about one’s own and the family’s future; also anxieties in respect to particular fears: a fear of the possible coming of fear, a fear of one’s own death and of the death of the close ones.
We have anxieties related mainly to the subject himself, anxieties about his own fate, fear of death or bankruptcy, various kinds of phobias such as claustrophobia, agoraphobia, fear of snakes and insects. Here also belong fears of disease, fears of being poisoned by food, and fears of the unknown which appears to threaten at any time and from all sides.
In such anxieties consciousness has limited role, the inner
120
psychic milieu is weakly developed and the capacity for inner psychic transformation is also very limited if not altogether absent.
At the lowest level we are dealing with a condition close to hysterical fear, without any stronger reflectivity, without the capacity for inner transformation or the formation of an inner milieu. This is related to a primitive stage in unilevel disintegration, usually with strong somatic components.
We observe on this level fears of external situations, of assault, of threat to life, of accidents, or economic insufficiency. Here belong such primitive phobias as the fear of being robbed shown by hiding money at home, searching for burglars under beds and in closets, etc.
Clinical observations indicate that with a high level of mental development of the individual such dynamisms as the third factor, subject-object in oneself, frequently identify with anxieties and fears. For example, in an existential anxiety or in anxieties concerning responsibility these two dynamisms do not, as a rule, prevent the experimental process or the decision for self-sacrifice and decisive action. In fact, these dynamisms enhance both the experiential process and the individual’s ability to take action.
On a lower level of psychoneurotic anxiety these dynamism; do not operate, and other dynamisms such as astonishment and disquietude with oneself are also inactive. The fears characteristic for lower level of development are combined with pathological processes which make conscious control impossible.
Examples of different levels of psychoneurotic anxiety are Case 3 (anxiety-obsessive psychoneurosis at a high level) and Case 4 (anxieties at a low developmental level).
(4) Psychoneurotic depression
Psychoneurotic depressions also involve different levels of functions.
The highest level of depressions is represented by a depression of existential and altruistic character showing concern for the other, while the lowest level is represented by sadness
121
and dejection centered primarily on oneself. These two levels of depression are best exemplified by two kinds of feeling of inferiority: one, a feeling of inferiority toward the external world whereby the individual becomes depressed because he perceives himself to be less fortunate than others, and two, a feeling of inferiority with respect to oneself related to an internal hierarchy of seeing in oneself the lower and the higher where by the depression is creative because the individual makes attempts to find ways of it.
At the very highest level of endowment and the nuclei of personality development, the depression would be expressive of a process of liberation and development of personality nuclei. It would reflect the person’s criticism of himself, some disquietude and dissatisfaction with himself, feeling of inferiority toward himself because of his own unfulfilled possibilities, guilt feelings, excessive tendency to self-observation and self-objectivity, an exaggerated influence of the “third factor” as expressed in self-denial or self-criticism. One of my patients wrote this about it: “How close are now my depressions, how far away the preoccupation with my own sensations, with my inner discomfort, whether psychic or organic. Something has fallen over, gone away. It taught me to be sad with the sadness of others, to be depressed with the depressions of others, to suffer with others. These depressions enable me to think differently, they expand my awareness to feel the `pain of the world.” This amounts to “clearing” the field for a new creative force of the individual. Symptoms of such depression are found among creative individuals, especially in art, literature and philosophy.
Experiencing the new in the form of deeper problems and of wider scope is a critical experience (meaning crisis) usually related to the experiencing of a hierarchy in the levels of interests and goals. This “new,” “different” and “deep” as a rule mobilizes creative forces. This is practically a universal phenomenon for individuals endowed with positive developmental potential. A deep experience of sadness and depression as a response to some kinds of reality activates powers affirming the existence of a higher reality together with powers needed to come to the
122
realization of that higher reality. Such depression is often followed by creative excitement, and contains elements for bringing to completion a creative effort. Representative types of this condition are, among others, Saint-Exupéry and Wladyslaw Dawid (1935).
At a lower level of depressive neurotic reactivity, we shall find ambivalent excitation, anxiety, depression, wherein any elements of creative inner transformation would occur rather marginally, without including the whole personality, being closed in a vicious circle of “pathological rumination.” There are paltry sadnesses, paltry worries, and paltry difficulties for which one does not see a solution. There is a fixation without an “upward” movement, without direction and without a hierarchy of values. There are no channels open for a developmental path leading up, i.e. toward multilevelness.
At the lowest level we find symptoms of hypochondria and of depression of a neurasthenic type. These are thoroughly uncreative symptoms of psychosomatic fixation to specific organs or groups of organs, accompanied by considerable narrowing of consciousness, a superficial intravertization, stiffening of inner attitudes, and inability for any inner psychic transformation.
Examples of the multilevelness of depression are provided by Case 6 where together with psychasthenia we observe a strong depression of an existential character and similarly in Case 2. An instance of depressions on a fairly low level is Case 1.
(5) Hysteria
At the present hysteria is symptomatologically different from the syndrome described in the nineteenth and beginning of the twentieth century. Despite the differences in description and usage we can differentiate in hysteria recognizable levels of functions.
On the highest level we would note a somewhat infantile symptom of creativity imbued with charm, psychical freshness, tendency for psychical erotization without stronger needs for-sexual life, tendency for sublimation, enchantment, ecstasy, em-
123
pathy and identification. Here we would have an excess of emotional sensitivity and imagination together with considerable creative ability. Such people are often called “interesting” because they are flexible, intuitive, direct, nontrivial, endowed with broad and changeable interests, at home in the world of fantasy and imagination.
At a middle level we would have a number of syndromes characteristic of hysterical conversion, with a high emotional sensitivity, weak analysis and weak reflectivity as well as weak inner psychic transformation. A good example is Case 7 where there are distinct symptoms of conversion, magical thinking activated under the pressure of strong basic drives (sexual and maternal). This corresponds to a process of unilevel disintegration.
At the lowest level we would have what is known as hysterical characteropathy, with symptoms of confabulation, lying, mythomania, primitive eroticism. We observe a facility to cry and to laugh, easily arising and easily passing pains in the heart and in the stomach, in most cases more faked than real. These symptoms are a means of half-conscious manipulation to get what one wants like money, promotions, concessions from family, lovers and others.
4. Psychoneurotic Dynamisms as Preventive and Immunological Factors
A closer look at psychoneurotic dynamisms through observation and analysis of the various forms which they take in development gives us an interesting insight into their preventive and immunological nature.
It is the task of a defensive strategy to get acquainted with the enemy, to produce protective mechanisms corresponding to the aggressive ones. For immunization it is essential to absorb a certain quantity of detrimental bodies, such that the organism, without being overwhelmed by them, becomes prepared to neutralize these foreign bodies by forming antibodies.
Similarly, in psychoneuroses we find some disruption, disharmony, disorder, or psychic disequilibrium which are common
124
to a great majority of psychoses; on the other hand, it is a distinctive feature of psychoneurosis that it involves hidden opposite forces, counteracting involutionary pathological dynamisms.
In a general outline of the aspects of positive disintegration, two traits are especially characteristic for psychoneuroses. One is an increased psychic sensitivity or excitability, the other is movement of the disposing and directing center to higher levels and the establishment of the inner psychic milieu in hierarchic order.
(1) Psychoneurotic sensitivity
Psychic overexcitability in relation to oneself and the environment is always one of the basic causes of inner tensions, conflicts with oneself and with the environment. It forces one to cut paths leading to multilevel positive disintegration.
Where there is sensitivity in respect to the growing inner psychic milieu then we observe growth of self-awareness, creative tendencies and in consequence specific changes in the perceptions of the external world and of the internal one as well. This then is the basic texture of positive transformations. Self-observation and the experience of oneself are the prerequisites of seeing others in their individuality and existential aloneness. Gaining in distance and objectivity towards oneself allow one to perceive the unique subjectivity of others. This process eventually becomes a source of motivation in development and is therefore called the dynamism “subject-object in oneself.” It leads to a need of transforming oneself, of gaining more control and self-determination. It develops a deeper understanding of others. One patient expressed it in the following way: “With my extreme sensitivity I am in such a cruel state of mental tension that I have only two solutions: to commit suicide or to find an effective way of changing myself.”
All this demonstrates preventive tendencies contained in various forms of increased psychic sensitivity, in the nuclei of the inner psychic milieu and the hierarchization of values, and in the nuclei
125
of inner psychic transformation. In most cases the preventive tendencies give rise to a creative tension and a sensitivity which inevitably discovers ways of channeling these tensions “upward.” All these forces, which, according to narrow one-sided scientific conceptions appear as “chaotic” psychoneurotic forces, represent protective, prophylactic dynamisms of considerable influence in development.
It is then of great importance that this be taken into account in the diagnosis of a patient’s “illness.” A diagnosis must, therefore, be detailed and specific in order to prepare the patient to accept his own constellation of creative and original elements of his personality together with so-called pathological inclusions. It is thus important to help the patient in organizing a more comfortable style of life, to enhance his friendships and feeling of being in touch with himself, because in this way one strengthens his prophylactic potential.
(2) Psychoneurotic “unrealism”
The reality function at a higher level is strictly related to a higher creative role. It also plays a positive role in the formation of a hierarchical development of values and activation of the personality ideal.
The Polish poet and playwright Wyspianski said about himself: “I am naught but a fantasy, I am naught but poetry, I am naught but a breath, but deep down there is the power of the spirit...” Kafka who seemed to be so far removed from the realities of life, nevertheless, gave in his writings a penetrating analysis of the everyday tragic reality of life in its anonymity, automatic routine, tragic antinomies. We see today the contradictions between statements of politicians and their subsequent actions, between the expectations of couples before marriage and the disillusionment and conflicts of their married life, between the display in the same show window of a picture of beautiful landscape with birds in the sky and hunting guns for sale.
One of my patients said this: “I am deeply affected by the, remarks of my family and friends that I know so little of the practical things in my life, and that it is so hard for me to stay
126
with it. Yet they do tell me sometimes that I do not neglect my duties and that all than I am supposed to do I actually carry out. Sometimes I think that if I were to strive to be more practical then my whole theoretical and practical structure would fall down. I am actually convinced that the essence of my activity in life must be in my higher reality.”
It appears that one cannot develop in oneself “higher reality” without at times neglecting the lower everyday reality. And it appears too, that sometimes separating oneself from lower levels of reality is a safety measure preserving man’s awareness and sense of integrity. It is a reaction of positive maladjustment which saves sanity by offering an independent sense of perspective.
(3) The prophylactic role of depressive and hypomanic states
Depressional tendencies as such are not necessarily a positive factor in development. However, when tendencies to depression are a function of the developmental potential, then depression becomes on occasion for the development of self-evaluation, of an existential attitude, and of empathy.
A depression marked by distinct elements of self-awareness expresses—among others—the feeling of one’s own limitations and deficiencies and at the same time the perception of the qualities and worth of other people. This recognition of the value of others and self-criticism have a very fundamental role in development. It promotes the dynamisms of self-control and of looking at oneself objectively and at others in their subjectivity (“subject-object in oneself”). It protects the individual in his relationship of “I-and-Thou,” i.e. in the development of conscious and controlled empathy [see Chapter 7, Section 3(4)1.
Hypomanic conditions, while co-existing with depressional tendencies, may be instrumental in playing a creative role in individual development. Individuals endowed with positive developmental potential utilize, so to speak, the nuclei of their depressive and manic states as modes of their personality growth. The depressive states are the means of “purification” of one’s tendencies. If the individual at the time of his depression is capable
127
to activate a state of sadness and distress in relation to others, then in the hypomanic state that follows after, he is able to mount considerable power of help and protection to others. By this he is safeguarded against adevelopmental forms of depression and hypomanic states. The manic states are a means of developing creativity, enthusiasm, inner movement “upward.”
If, therefore, there exists some positive developmental endowment, then, give appropriate environmental conditions, we can find in hypomanic-depressive conditions all the necessary defensive and immunological factors protecting against more severe mental disorders.
(4) Prophylactic role of isolation and quietude.
In the very tendency for isolation, quietude, concentration and meditation, and even in a tendency for ecstasy, can exist some very constructive prophylactic and protective forces. For example, in an hysteria with more pronounced nuclei of multilevel disintegration, the tendencies toward periodic isolation, loss of interest in actuality, lack of response to external environment, tendencies for meditation or ecstatic states, are the very conditions which may contribute to the development of a reality function at a higher level and to the growth of a hierarchical inner psychic milieu. These conditions allow to discover and to realize higher forms of reality, such as, for example, the reality of genuine mystical experiences.
As we have pointed out previously, an accelerated development of abilities and talents appears at the borderline between unilevel and multilevel disintegration. The psychical tension rising at this time within the inner milieu provides favorable conditions for the formation of new outlooks, concepts, and attitudes connected with an increased need for non-adjustment to the actual situation, and with a parallel drive for adjustment to new, striking, usually higher level phenomena, such as a sense of growing, a clearer vision of the ideal, an increase in the ability to experience contemplative contents and actual increase in experiences in this respect. In the stages of meditation, first in the growing calmness and recollected concentration there is a presentiment that new
128
important contents are going to arise; in deeper meditation this new reality becomes alive before the mind; and ecstasy is a clear vision of a transcendental reality.
Many of my patients told me that as a result of practicing meditation, or of periods of solitude, their relation to themselves and to the external reality underwent a positive change. The feeling of “going insane” from tensions beyond control subsides, the tension drops and there is a “temporary” integration of a global character. Periods of isolation, meditation and contemplation of beauty together with his artistic efforts marked the beginning of Clifford Beers' recovery from a grave psychosis (Dąbrowski, 1967). Jan Wladyslaw Dawid saved himself from prepsychotic condition and suicide by reaching to meditation and a serious study of mystical experiences (Chapter 10). Isolation, meditation and creativity were the essential factors in the life of Kierkegaard and Kafka by which they “tamed” their depressions and anxieties bordering on psychosis, and by which they turned them into the very dynamisms of their development and creativity.
(5) The prophylactic role of positive regression
Children or young men of very high sensitivity with possibilities for positive development, are often found to withdraw before excessively strong collisions with the brutal external environment. A retreat to earlier periods, to childhood, whether in imagination or in reality, a retreat to conditions of quietude, to the world of fairy-tales and fantasy, to a period of creativity, to a warm family atmosphere of affection and childhood dreams, may provide the necessary forces for immunization against strong difficulties. A child who is emotionally sensitive, has a vivid imagination, is shy and manifests a preponderance of inhibition; a child capable and ambitious but with a dominant tendency for withdrawal will tend to be ambivalent: on one hand, it will be his desire to be noted, to gain strength, and on the other hand—and often more distinctly, he will tend to retreat in thought and imagination to a world of undisturbed joy, sincerity and spontaneity, which characterizes many a childhood period. There, he regains resources and energy to measure up to a more “grown up” world.
129
These various forms of non-adjustment to actual reality, to the “grown up” world and to excessively severe conflicts, are expressive of a tendency for positive maladjustment. At the same time there is a tendency to adjust to that “which ought to be,” which is a pursuit of the ideal (Dąbrowski, 1964). Towards this end, it may be found necessary to go back and retreat to the period of greatest inner comfort wherein the psyche becomes saturated with the stimuli of a positive developmental character, as a defense again against premature and destructive stresses.
(6) The prophylactic character of different forms of hereditary endowment.
We now turn to various forms of hereditary endowment in the light of their protective, prophylactic and developmental character. In this category are special abilities, talents, and various kinds of sensitivity to internal or external stimuli related to some psychoneurotic dynamism.
The nuclei of the inner psychic milieu provide for its development into a multilevel structure. These nuclei appear together with abilities to transform different forms of psychic overexcitability into multilevel processes, and even to transform talents not only by making them richer and deeper but by combining them with the instinct of self-perfection.
The interlocking relationships between different developmental nuclei integrated into one vector of a developmental instinct play an essential role in the transformation of external and internal stimuli into stimuli operating on many levels. These couplings determine a closely woven activity of different forms of enhanced excitability, especially emotional, imaginational and intellectual; they also determine how to make use of the positive aspects of sensual and psychomotor overexcitability by subordinating them to the other three higher forms of overexcitability.
When the psychomotor and sensual overexcitability come under the control of the other three forms of overexcitability they lose their isolated character and leave their single plane of operation. Affective, imaginational and intellectual overexcitability have a higher potential for the evolvement of multilevel dynamisms. Thus
130
psychomotor overexcitability is transformed into a strong dynamic ability of planning and carrying out one’s goals, while sensual overexcitability develops into a hierarchical sensitivity acting towards seeking delights on higher levels of experience (many mystics show strong sensuality transformed by the power of their emotions and striving for self-perfection).
One of my patients described these processes of transformation as they occurred in her experience: “I feel the activity of the same tendencies as before but now on a totally different plane; luckily, somewhere I have lost my outbursts of anger, discontent, violent movements. I am told, and I see it too, that I am, as before, dynamic, quick to make up my mind, a good planner and a good organizer, yet all these activities are a part of a different, higher reality which has for me an altogether essential significance.”
Miguel de Unamuno, for instance, in the course of his own development saw the necessity for coming in touch with transcendental reality without losing the richness of sensual concreteness.
These processes develop the dynamisms of autonomy, authentism, empathy and responsibility. They enhance the reality function on a higher level, the hierarchy of values and the personality ideal; they precipitate the growth of the disposing and directing center at a high level and the growth of inner psychic transformation. They activate education-of-oneself, autopsychotherapy and develop faculties of meditation and even ecstasy.
If someone is “in touch” with these higher dynamisms (meaning that their presence and activity is felt although they have not yet fully evolved) then his depressions, anxieties, obsessions are somehow under their control. They channel and sublimate these states and extract their positive value thus changing them from pathological into developmental processes.
One patient wrote this in his autobiography which illustrates this point: “From these ‘spiritually bleeding' struggles emerges a new force, a new truth, a new power which directs me. I feel that my stored-up experiences, sufferings, disturbances have been collected together and employed by ‘new', higher forces which
131
changed them, molded them, and have given them a new meaning in my growth. How blessed are these transformations.”
The highest factors of hierarchical polarization gradually begin to mark their activity, such as the highest empathy and the recognition of the highest values of one’s personality, such as the awareness of approaching the ideal and the attitude of deepest humility. This is reflected in the prophylactically advantageous structuring of particular psychoneurotic syndromes. The states of anxiety gain a predominance of altruistic and existential components. The same goes for states of depression. In paranoid-like states the condition of suspiciousness is often overcome by growth of empathy. Obsessions expand from their narrow and rigid forms into self-sacrifice and struggle for a worthy cause, obsessions of love and work or self-perfection attain a higher level of empathic insight, they also gain in enthusiasm derived from a reality of a higher level.
Psychasthenics express their creativity in the area of new concepts, new images, new psychological insights by deriving their stimulation from a reality of a higher level. The localization of the most important dynamisms on a higher level of the reality function gives the patients the power of creative systematization. In consequence, in spite of their lack of adjustment to everyday reality (reality function on a low level) they have now a creative and empathic “protection” against psychosis and involution.
Psychoneurotic hysterics may come up with creative solutions which transform their neuropathic behavior into processes of deep identification with chosen heroic figures expressed in highly artistic forms. Hysterics are usually sensually excitable, i.e. they readily respond to concrete sensory stimuli. This “concreteness” does not disappear but favors the need to preserve individuality, exclusivity, also on a higher level. At a lower level of hysteria we observe play-acting or primitive dramatization, but at a higher level it becomes the “dramatic charm” of great artists, especially actresses (sublimated hysterical traits).
In the course of development only insignificant traces are left of the lower levels of hysteria. The individual develops his en-
132
hanced emotional overexcitability, high level of “concreteness” in the approach to life’s problems, empathy, and a capacity for meditation and ecstasy which preserve him from psychosis and involution because they allow him to take great steps forward in his individual evolution. Great syntonic and empathic reactions characterizing the conditions of depression and sub-depression often express the elevation to a higher level of human feelings, understanding, respect, humility, etc. These forms of depression and existential anxieties, altruistic anxieties, favor the growth of deep empathy, deep relationship between “I” and “Thou.” Such developments have strong prophylactic value against egocentrism, psychopathization, and paranoidal tendencies. One of my patients said: “I was unable to reach higher levels of love, friendship and sacrifice without first developing—during my sadnesses and depressions—humility and a feeling of inferiority.”
An example of these transformations is Case 6 which represents clearly a transition from anxieties concerning his mental health and the possibility of going insane to much more difficult and complex concerns, tensions and anxieties about others, and about the highest values. We see that too in the case of the young priest (Case 3). It was fairly easy to help him understand that what was necessary, in his high but somewhat one-sided way of development (motivated by feelings of guilt, sin and striving for salvation) was social involvement in concrete pastoral work for others.
Against the background of mental tension which accompanies disintegration of primitive structures, there is, then, the concomitant tendency to transcend the routine stereotype in hypomanic attitudes through a search for channels in creative inventiveness, through richness of association and improvisation resulting from multidimensionality and strength of emotional stimuli. The quote from Weininger given earlier is a good example (p. 61). One Polish poet expressed himself thus: “I don’t live and I don’t want to live, but I'll say more, I'd live but a beautiful life, I spit on piggish existence.” In another way if Dr. Janusz Korczak (p. 97) did not find more of what in his life pulled him to grow he would have committed suicide.
133
(7) Pathological versus psychopathic structures
Pathological tendencies, even of containing some positive elements, do not possess any discernible trends leading “upward,” and, therefore, by themselves do not possess any possibilities of positive (i.e. developmental) changes. An individual who undergoes very severe tensions and does not see a solution to them, does not see their value in self-growth, does not have love and empathy, is thus deprived of prophylactic elements that would save him from suicide or mental illness.
Inner psychic transformation together with other developmental dynamisms prevents the realization of pathological tendencies leading to an unconscious disintegration of development.
The phenomena of positive disintegration, so characteristic in psychoneurotic processes are very different from symptoms of psychopathy, mental retardation, or some paranoidal syndromes. The latter cases, in both psychopathological structure and process, shall be discussed (Chapter 9) in terms of the phenomena of rigid primitive integration, fantasy or delusions of a rigid type, stemming from a lack of an inner psychic milieu and any possibility of inner psychic transformation. If someone does not see himself and his deficiencies, if he is a rigid egocentric, if his inner psychic milieu is not developed, if he has no inner psychic transformation (and hence no possibility of transcending his psychological type) then such a man transfers his irritations and misunderstandings onto the world and people outside himself. In his mind, his difficulties always originate in the ill will of others. He then develops aggressiveness, suspicion and a desire for getting even or getting his revenge for transgressions not committed by those who are his victims. This is always the case with great and famous psychopaths in history. This is the case with small psychopaths and individuals with paranoid like traits, such as suspicion arising from a concern to protect one’s own business, irritability, a need to underline one’s own importance or even greatness. If one is without an inner world, without an inner psychic milieu, then all conflicts and matches are fought between the external world and the psychic surface of the individual. Since he has no inner psychic transformation there is no penetration into his psyche.
134
In all such disorders we shall find a preponderance of external conflicts with an apparent absence of inner conflict. We will observe in these types an excessive fixation to the external milieu and an inadequate understanding of that milieu. Hence will follow intrigues, jealousies and distortions in respect to that environment. There will be a concurrent lack of self-awareness, inner psychic transformation and responsibility. We shall observe behavior “true to type” without any ability for identification—even partial—with people of other types, resulting in a lack of deeper syntonic and empathic contact with others.
It is precisely here that we encounter a definite and specific boundary between, on the one hand, psychoneurosis as a positive, creative developmental process leading to the formation of protective and prophylactic conditions of growth, and on the other hand, a nondevelopmental structure without any inner psychic milieu, as in psychopathy and the processes of negative and involutive disintegration characteristic of most psychoses.
Even phenomena which are definitely “pathological,” such as somnambulism, may have hidden protective elements operating through the release of consciousness from the excessive burden of intense experience, and by seeking refuge into the sub-conscious release tension, and permit—in the most difficult periods—a less disorderly management of one’s own strength until such time as psychosomatic equilibrium is recovered (cf. case 5, Irene). Many individuals enter somnambulistic states following grave experiences because they are not capable to experience their tragedies consciously and with a continuity. A somnambulistic “interlude” may well be a mechanism of protection against a schizophrenic split. In contrast such psychoneurotic “split” of personality gives relief and rest from too strong and constantly present stimuli. This then may well be a mechanism of prophylactic escape before an overload of suffering.
(8) Summary
We have briefly considered some general problems of unilevel and multilevel disintegration as processes of psychoneurotic lo-
135
osening and breakdown, and also as a global multilevel process which leads to integration at a higher level and forms creative and prophylactic forces.
The main dynamisms of the inner psychic milieu such as disquietude or dissatisfaction with oneself, “subject-object in oneself,” the “third factor,” inner psychic transformation, attitude of responsibility, the localization of the disposing and directing center at a higher level, and the development of the personality ideal, play a basic role in the development of objectivity with which a person begins to see himself, as well as the parallel increase of syntony and empathy towards other people.
To see clearly one’s own positive and negative sides and to experience one’s growth gives great possibilities of a different attitude toward such of one’s tendencies which until now were either regarded as pathological (excessive sensitivity, disquietude, depressions), or maladaptive. With a change of attitude one begins to see the positive role of these tendencies. One sees that they help in development by serving a prophylactic function. They fulfill this function, among others, by releasing uncreative tensions—tensions that followed from uncritical acceptance of schematic explanations of human behavior. This leads to the removal of blocked and unchannelled stresses, and to the resolution of these disturbances at a higher level through an understanding of the multilevel character of human behavior. In consequence there is a marked increase in tolerance and responsibility.
It is through the formation of the dynamisms of a higher level, with the accompanying transformation of one’s own psychological type, that there are being formed better conditions for the protection of one’s psychically healthy development. Thus the defense (protection) and prophylaxis against serious mental disorders or suicide occurs through development itself.
Let us summarize the problem of protection and prophylaxis by listing characteristic psychoneurotic dynamisms.
1. The nuclei of positive hereditary endowment, in the form of psychic overexcitability, (cf. Chapter 1) nuclei of multilevelness, general and special abilities and talents, etc., de-
136
termine, on the one hand, accelerated development through positive disintegration, and, on the other hand, build protective and prophylactic forces in the form of mental and emotional plasticity, hierarchization of levels of reality and levels of values, and the need for the realization of personality and its ideal.
2. The psychoneurotic processes of positive disintegration contain in themselves the dynamisms of autonomy, authentism, and aspirations for developing original approaches to reality; in other words, they carry the potential for transformation of internal and external stimuli. The dynamism of transformation activates and develops protective and prophylactic forces against mental stagnation, stereotypy, and automatism.
3. Psychoneurotic experiences, together with conscious inner psychic transformation, by being essentially developmental, create basic immunological dynamisms against both psychotic dissolution and negative regression.
4. By providing appropriate assistance for the development of the personalities of psychoneurotics, their depressive syndromes can be used as a phase of psychic transformation, development of self-control, of objectivity, etc., which will shape and rectify subsequent states of excitation (such as greater enthusiasm for friends, great ideas, service to others). By means of conscious autopsychotherapy in psychasthenia, the reality function at a higher level can play a creative, and thus, therapeutic role in the development of the personality of psychasthenics. The obsessive element in psychasthenia, or in true psychoneurotic obsession can be directed towards the elaboration of a stable attitude of positive determination and constancy of feelings, thereby channelling it through developmental dynamisms. When obsessions are channeled through understanding and experiencing their positive aspect then they gain more of positive dynamics in development over strong fixations which block development.
In psychoneurotic anxiety, the protective and developmental dynamisms are expressed in terms of the richness
137
of existential attitudes, in the subtlety characteristic of anxiety states, and in the introversion and specific creativity related to this type of neurosis.
Psychoneurotic infantilism may also provide an opportunity for helping the individual by helping him to understand the positive nature of his personality characteristics and by awakening his potential for manifold creativity. Even certain dystonic traits in a somatic neurosis may be channelled through a slow development of self-awareness on the basis of a proper interpretation of disturbances in inner sensations.
138
CHAPTER VIII
PSYCHONEUROTIC OBSESSIONS(1)
1. The Place of Obsessions in Positive Disintegration
In the previous chapters we have been trying to demonstrate that psychoneurotic processes—particularly those that are more complex—indicate the presence of higher dynamisms allowing accelerated development. We do not mean by this that maturity is achieved sooner in life but that the individual evolution has a greater chance of reaching the advanced stage of multilevel disintegration when the synthesis and unification of different psychical structures and dynamisms begins to take place. In this sense these higher dynamisms of accelerated development are creative. They are creative because internal conflicts, depressions, inhibitions, states of anxiety, and obsessions express the transcending of lower levels towards higher levels of development. Obsessions in one form or another appear to be a phenomenon associated with the incapacity (temporary or chronic) to break through to the higher levels. Obsessions would thus appear as a predictable phenomenon at such stage of development when a process of positive disintegration is not completed, as we shall try to demonstrate.
2. Classical Theories of Obsessions
Pavlov (1941) tried to explain some obsessions as a memory of a painful experience which is so strong that no retraining by means of conditional reflexes can change it. Other obsessions were in his opinion related to a permanently morbid imagination,
_____________________
1. Paper presented at the Honorio Delgado Congress of Neurology and Psychiatry, Lima, Peru, November 1970.
139
or to a “vicious circle”: the more someone tries to free himself of his obsessive symptoms and the more he tries to inhibit them, the stronger they become. This, of course, explains better the persistence of obsessions rather than their origin. In no way was thus Pavlov able to account for such psychoneurotic; complexes as religious obsessions, obsessions concerning problems of identity, existential obsession, obsession of sin and guilt, obsessions of self-perfection, or obsessions of absolute love found in people like Kierkegaard or Saint-Exupéry. Yet such obsessions and psychoneurotic processes are by far more complex than experimental neuroses in animals, and constitute the majority of cases.
Janet (1926) defined obsessive neurosis as a more intense and uninhibited activity of lower functions to compensate the defective activity of higher mental functions. In consequence psychological development is arrested. The failure of the higher functions thus to exercise control over individual’s thoughts and to guarantee that he perceived himself and his environment realistically, releases the emotions from under control and leads to mental disorganization. Hence obsessions, anxiety attacks, compulsions and phobias.
This view is hardly more adequate than Pavlov’s. Psychoneurosis is a process by which higher functions are developed not lost. These higher mental functions become very active in obsessive individuals as in the case of Kierkegaard, Proust, Kafka, or Korczak, to quote some eminent examples. We cannot say, therefore, that obsessions represent a greater compensatory activity of the lower functions while the higher ones are defective, and that a psychoneurotic individual, and an obsessive one in particular, has a deficiency in his reality function. We have shown in the previous chapters that mental functions together with the reality function operate in the majority of psychoneurotic individuals more strongly on a higher level than on the low level.
Kretschmer’s (1931; 1960) explanation of obsessions as rooted in abnormal sexual constitution does not seem to be more helpful either. In very many cases of obsessions sexual obsession is really negligible.
140
According to Freud (Jones, 1920; Freud, 1924) the pathogenic factor in obsessive-compulsive neurosis is self-accusation and self-reproach which are repressed and date back to childhood. They are always related to sexual inclinations or sexual activities. They are an expression of a regression to the sadistic-anal period. The obsessive-compulsive symptoms are a symbolic expression of conflicting forces, and, therefore, of uncertainty and insecurity (the need to act clashing with the incapacity to act).
All these theories treat obsessive individuals as less developed than the integrated individuals who function well in life and do not suffer any obsessive and compulsive thoughts. Such individuals on close examination are almost always primitively integrated, they have no feelings of guilt and they do not suffer from internal conflicts because they have never broken out of their rigidly defined typological structure controlled by basic drives. These individuals are less developed than the obsessive ones.
3. Clinical Cases of Psychoneurotic Obsessions
(1) Moral obsession
S.M., the young student of art already described (Case 6, p. 95a), suffered from obsessions of personal responsibility for the death of those who died in the war and especially in the Warsaw uprising of 1944. His preoccupation with self-perfection, with moral problems, with the meaning of art and the meaning of man’s existence had the character of obsessions of great tension so that he feared becoming mentally ill. His relations with his parents were very good and on examination by dream analysis and free association appeared to be free from subconscious repression. How then does one explain his obsessive reactions? Pavlov with his theory did not seem to be interested in such complex human dynamisms. There were no unresolved sexual conflicts in S. M.’s case.
(2) Obsession of self-destruction
S. Mz. (Case 2, p. 34) was a woman who suffered from suicidal obsessions and recurrent thoughts of going insane. She
141
trying to find the evidence that she was schizophrenic because the certainty of being mentally ill would have given her relief. It will be recalled that she suffered immensely after the death of a man she loved, because she could not accept his death.
S. Mz. Shows the need for exclusive love. She cannot reconcile herself with the death of those she loved (her mother was dying). When death destroys a beloved person this gives rise to an obsession of rejecting the fact and as a secondary reaction to the desire to destroy oneself through mental illness or suicide. This is why she as much as demanded from me the worst prognosis for herself and why she was developing the dynamisms of her death instinct.
This type of reaction is frequently encountered in people who are very sensitive, hurt, humiliated (as she was in her working environment), who do not see any way out of their situation. They then want to complete the job of destruction already begun by fate.
Such obsessive-compulsive processes arise in face of the impossibility to solve the most fundamental problems of life, as a result of a hopelessly grave emotional and mental struggle. This again is a case when the classical theories of obsession do not offer any useful explanation.
(3) Ambivalence
Case 10. S. was a young man 25 years old. He was very timid, emotionally inhibited and suffering from anxiety. These are signs of an emotional overexcitability. His movements were nervous and quick, he was biting his nails and his lips. He talked fast and a lot. These are signs of psychomotor excitability. He was excessively preoccupied with his health. His emotional inhibitions and crises tended to be transposed into somatic reactions. He had internal psychic hypertension. There was ambivalence in his feelings since he alternated between being excited and being inhibited.
He was continually tormented by scruples and blasphemous
142
thoughts which would appear during prayer. He felt compelled to offer something sacred to Satan. He was caught between accepting these obsessive thoughts and trying to drive them away through magic. During these obsessions his will was paralyzed, and they could arise at any time whether he was talking with someone, riding a bicycle, or reading. These thoughts, however, were more frequent at night and were often related to masturbation.
One can distinguish in this man three trends. One is his normal daily life and normal attitude towards his tasks. Another is a tendency toward a higher moral development and toward self-affirmation. And the last is a tendency toward self-negation, when he condemned and rejected himself for his obsessions. In this he could only find again an affirmation of himself on a lower level by means of masturbation.
S. represents a case of development on the borderline of unilevel and multilevel disintegration. This in-between stage is replete with tensions and the transposition of emotional experiences onto the autonomic nervous system. His inclination to use magic and ceremonies as a means of defense against obsessive thoughts are characteristic of unilevel disintegration.
The prognosis in such a case is not bad, but is not too good either. It is true that there is a great conflict, great tensions and also a desire to reach a higher level of development. But on the other hand, the positive developmental potential appears somewhat limited (lacking primarily in intellectual and imaginational excitability and in special talents). The principal dynamisms of early stages of multilevel disintegration do not yet appear to strongly mark their presence.
The recourse to magical solution is an expression of the state of “suspension” between different levels. It occurs when one does not have sufficient strength to establish oneself firmly on the higher level, nevertheless there is enough mental and emotional power and sensitivity to feel a distaste toward oneself. The balance of power between forces pulling “up” and those pulling “down” leads to tensions absorbing the whole psyche.
143
In consequence the individual is beset by unceasing obsessions since his psyche cannot become in any way organized because of the tensions that tear it apart.
(4) Obsessions of death
Case 11. Here is a transcript of the first session with one of my clients suffering from obsessions of death. This man was 55 years old and was a well-known scientist.
C.: “I have not come to see you as a patient. I heard about your approach and so I would like to talk to you to have an exchange of opinions on a problem of your interest, that is, an appropriate attitude toward obsessions.”
K. D.: “Please, go ahead.”
C.: “To tell you about my obsessions. I have many obsessions and they give me a lot of tension. I am suffering from obsessions in relation to my family. I feel that the members of my family are dead. I do not see them as dead but I know that in my imagination they are dead. This makes me terribly tense, I cannot sleep, and I am very upset. The awareness of senseless killing pursues me obsessively and upsets me emotionally. I can neither get rid of these thoughts nor can I divert my attention from them. I often think of the thousands of people murdered in concentration camps and prisons. These thoughts trouble me while I am working. They turn me away from what people call God’s justice. Also when I see the statistics of the numbers of people killed in car accidents I have obsessive thoughts. I see corpses spread along highways.”
“The question of death troubles me every night. My death does not worry me at all. It is rather the death of creative, valuable and innocent people which bothers me, and also the death of the members of my family. Often in my dreams I see thousands and thousands of tombs and hearses on their way to the cemetery. I know that this is fantasy, a tragic fantasy, but I see
144
these pictures very vividly. And then I often ask myself how must I behave to face death, and will I be able to help man become immortal, and how is man going to transform his body and his mind to become immortal.”
K. D.: “How long have you had these thoughts and feelings?”
C.: “Since my early childhood. At that time these obsessions took childish form. I remember one very clearly, a vision of corpses being tossed into their graves. I woke up feeling very anxious, and I could not get back to sleep.”
K. D.: “Did you ever consider these thoughts to be unhealthy?”
C.: “Yes, for a number of years. I even consulted a well-known physician but his explanations did not do anything for me. His advice was useless. Now, I do not think that my obsessions are pathological. Actually I would say that without these thoughts I would feel psychologically poorer and that my power of thinking would be weaker. According to my experience, obsessions similar to mine are given to some individuals so that they could understand the mystery of death. I find it queer that such cruel things are taking place on earth, that there is despair, and that people call it normal. I find it strange that they can go through these awful events and keep on living. They really must have a strong instinct of survival because otherwise they would not be able to resist. But resist what? I believe that very often it is useless to resist.”
K. D.: “I would like to ask you one more question. Do your relatives or close friends who are intelligent and can be said to think objectively, consider that your preoccupation with those ideas makes you more stereotyped and less productive?”
C.: “No, from such people I have not met with that kind of a reaction. It is rather the opposite.”
Individuals who like this man have an excessive emotional
145
and intellectual sensitivity, whose consciousness could be called “overeducated,” and which is at the same time alterocentric, are subject as a rule to this type of obsessions. The intensity of their experiencing, the pathos of their empathy, their inability to accept standard explanations of existential problems (the meaning of the existence of the world, the meaning of life, the meaning of death, the existence of injustice) cause and we may add—must cause—obsessions, depressions, states of anxiety. Alleviation, or disappearance of such obsessive processes can come about only when satisfactory solutions to these existential problems are found, either through deep friendship and understanding by close persons or a wise and insightful therapist.
I want to underline that no great human thought or deep emotion can be completely free from being obsessive. Kierkegaard’s love for Regina Olsen, or the love between Romeo and Juliet display obsessive traits. The same phenomenon occurred with one of my patients, Mrs. S. She was very conscious of her husband’s possible death, since he suffered from serious heart trouble. This thought and feeling filled the last years of her life. She saw in the persistence of this thought the indication that if her husband dies the only sensible thing for her is to die too. In the end, when her husband died of heart attack, about fifteen minutes later she took an overdose of drugs and died
4. Obsessive Processes in Creativity
Quite often an act of creation is the result of an obsessive process. The search for a suitable expression, the striving for perfection, the search for the one idea that would bring together loose ends and pieces, the search for solution to paradoxes whether of thought or of life, are characterized by an obsessive tenacity and very often precede a new work of art, a poem, a piece of music, a scientific discovery, or a social reform.
Michelangelo, for instance, was haunted by the idea of transforming a mountain which he could see from his house, into a gigantic sculpture that could be seen from afar (an early
146
version of Mt. Rushmore). Marcel Proust wanted to “bring back to life” close persons that have died (especially his mother). He wanted to achieve this by pouring life into these persons in his imagination, and by emotional and intellectual concentration. These persons would then “appear” in response to this call of affect stored in memory. Proust suggested that people around him do this too. It was clearly an obsession with him.
Miguel de Unamuno was deeply affected by the realization of the existence of tragic antinomies in human life as something essential for growth and yet impossible to resolve. The experience of these antinomies which evoked in him obsessive reactions, depressions and anguish, became a motivation to turn in the direction of transcendence in the hope of resolving them there.
Chopin’s Prelude No. 15 is an excellent example of a musical expression of an obsessive emotion.
5. Janet’s Classification of Obsessions A New Interpretation
Janet distinguished five categories of obsessions as given below. We shall look at them in turn and try to explain them as phenomena of positive disintegration.
(1) Sacrilegious obsessions and impulsions.
(2) Obsessions and impulsions of criminal content.
(3) Genital and sexual obsessions.
(4) Obsessions of shame in relation to one’s body.
(5) Hypochondriacal obsessions.
(1) Examples of sacrilegious obsessions. A man 40 years old has lost within two years his father and his uncle. He loved them both very much. He developed an obsession in which he saw the dead bodies of these two men soiled with their own excrements.
A young girl kept seeing in her mind male genitals. This made her extremely unhappy and desperate because this recurring image was humiliating her sense of chastity which was
147
sacred to her. She said that it was the devil who was pushing her to have such thoughts because he wanted her to be damned.
Often religious persons have blasphemous thoughts which are aggravated by the accompanying thought that God is responsible for their having these thoughts.
In most such cases the individuals subject to these obsessive thoughts are very sensitive and excitable emotionally, sexually, and in their imagination. They experience conflicts, they revolt against situations with no solution, they have feelings of guilt and often suicidal thoughts and inclinations (suicidal attempts). Also at one time or another these troubles are transferred to the autonomic nervous system tipping it out of balance (cf. Chapter 4). They appear to be caught between two levels: unable to leave one and incapable of reaching the other for good. Those ascents and descents between the two levels are accompanied by rich associations and impulsions demonstrating the strong ambivalence active in these people who are not in harmony with themselves, their hierarchy of values and their environment. It is this ambivalence which is expressed as an obsession and which indicates that these people are as if stuck on the borderline of unilevel and multilevel disintegration.
(2) Obsessions and impulsions of criminal content are often related to moral preoccupations. For instance, a man sees a lady sitting on a bench in front of a church and the thought of doing something violent to her crosses his mind. Another man is afraid that if he does not control himself he could kill people with a knife. A woman imagined herself cutting her daughter’s head and throwing it into boiling water.
Janet included in this type of obsessive thoughts also suicidal attempts and genital compulsions arising in some people when they come close to other persons.
This type of obsessive-compulsive reactions is usually explained as a transference of an unconsciously repressed aggression. This is often true. But it is also true that people experiencing such reactions, as in the examples above, rarely commit crimes. However, those suffering from suicidal obsessions are more likely to commit suicide. If there is a question
148
of an aggression then it is turned against the person himself in order to save others (Dąbrowski, 1937). But even more often a closer examination does not reveal aggressive feelings towards close persons but instead feelings of anxiety for them, feeling of guilt that not only they cannot be protected but have to suffer aggressive behavior, impatience, irritation. In this way the person’s aggressive and negative tendencies are being exaggerated to the fantastic image of being criminal tendencies.
It is thus more often the case that obsessions of criminal content spring from an “overeducated consciousness,” a consciousness which in its refinement amplifies the negative like an extremely sensitive galvanometer. Working only as an indicator such consciousness lacks the psychological mechanism that would interpret these reactions and place them in a meaningful context and trim them down to the right perspective.
Persons with this kind of obsession have rich and often very creative associations. Thus the obsessions of the possibility of committing an unethical, or even a criminal, act, never, or almost never, represent a real possibility of it being carried out. The states of anxiety may be very intense although they have no relation to the possibility of the crime being committed. The same phenomenon occurs in “obsessions of guilt” where no actual guilt can be recognized (saints). It is an “overeducated consciousness” accusing itself of uncommitted wrong.
Such obsessions can also appear in individuals on a lower level of development, i.e. unilevel disintegration. Here these obsessions may be an expression of a “condensation of experiencing,” excessive “unilevel saturation” as a consequence of being unable to sublimate obsessive contents. A sublimation or transformation of obsessive contents is possible only with the appearance of multilevel dynamisms which by building a hierarchy of levels of mental processes introduce the means of controlling the processes on one level by those of another. In a unilevel inner psychic milieu there is no other plane of mental activity strong enough to exercise such control, as for instance to make the obsessive contents yield to a stronger and more constructive interest.
149
The explanation for these obsessions is the same as for those o sacrilegious content. We may add here that ambivalence indicates that a disposing and directing center is not clearly active whether on a lower or a higher level. When the disposing and directing center operates on a lower level (when in fact it is indistinguishable from one or another basic drive) then no ambivalence, no conflicting tensions and no obsessions are as yet entering the picture. When the disposing and directing center is established on a high level then obsessions like those described appear no more . It is the lack of possible developmental solutions toward a higher level of development, or lack of possibility of negative regression to primitive behavior on a lower level that gives rise to great tensions and often intense obsessive-compulsive reactions.
(3) Genital and sexual obsessions. We shall not deal with these particular obsessions in detail. They overlap the first and the fourth of Janet’s categories and often appear on the borderline of psychoneurosis and psychopathy. Some of the obsessive dynamisms of this category have been described with the first (sacrilegious obsessions), and some will be described in the next section because they come closer to psychoneurotic obsessive dynamisms.
(4a) Obsessions of shame in relation to oneself. These obsessions express scorn towards oneself, moral discontent with oneself and putting the blame on oneself. Individuals who are persuaded to accept that their symptoms are abnormal and denote illness become used to evaluate their behavior as inappropriate, bad, negative or immoral. They do not cease to accuse themselves and find it justified if they are humiliated. They are full of uncertainty, hesitation and suspicion regarding themselves, and they strive to change their personality. To this group belong also those who are tormented by scruples of lack of love for their fiancées and yet in fact do have great love. Such individuals almost invariably see moral love as essential. The moral component is evidenced by their feeling of inferiority, feeling of responsibility, expectation to be em-
150
pathic on their part, which indicates the lack or at least a weakness of egoism.
Very often in this group one finds also an obsessive tendency to over evaluate others. According to Janet this is an obsessive attitude of shame. According to modern parlance this is hero-worship by weak sand inferior individuals. To accept Janet’s: idea would mean to conclude that the more individual feelings are refined, penetrating, reflecting the process “subject-object in oneself” the more they are pathological. In the context of positive disintegration an obsessive tendency to over-evaluate others is an expression of a high level of development at the stage of spontaneous multilevel disintegration. S. M. (Case 6), S. P. (Case 3), and all instances of cases of experienced inferiority and shame are clear examples of an obsessive tendency to over-evaluate others as a part of the growth process involving development of a more objective attitude towards others. This involves not only feelings of shame and guilt or inferiority towards oneself but also such important dynamisms of multilevel disintegration as astonishment with oneself, dissatisfaction with oneself and positive maladjustment towards oneself and the environment. The symptoms of these processes may be considered negative in therapy but only by those who do not want to be involved in the study of the multiple complexities of mental growth.
(4b) Obsessions of shame in relation to one’s body. One can distinguish here shame towards the body as a whole or towards its specific parts. Janet considered the refusal to take food a dangerous obsession expressing shame towards the whole body. Yet this is nothing more than “anorexia nervosa” and we have discussed it in Chapter 4 (p. 60). Other obsessions are related to a rapid growth of the body, disproportionate growth of legs, arms, nose or ears as in adolescents, which result in tendencies to blush. One may include here cramps seizing writers' hands which often arise as a result of an anxiety concerning the quality and adequacy of their writing, or even perceiving writing as an inappropriate activity. Similar mental inhibitions
151
or mental “convulsions” in the form of genital obsessions can cause impotence in men.
Most of these obsessive reactions appear in the course of development as a function of gaining a higher and broader perspective of inner growth. This unfolding of an authentic potential for development associated with tensions of anxiety, shame, feelings of inferiority in relation to oneself and to others constitutes the process of spontaneous multilevel disintegration.
Here is now an example drawn from the autobiography of a male patient, age 34. This example illustrates the developmental direction of obsessions of shame in relation to one’s body and its parts.
“I love animals very much, but only the calm and non-aggressive species. I do not like the bloodshot eyes of a dog, his tensed back in readiness to fight, or when he hunts for food. I hate the lack of inhibition in the sexual acts between animals. I resent the shame it gives me to have my own genital organs, and they are so close to the anus. I do not like primitive temperamental activities so linked with the automatism of the body. How far are we, indeed, from being able to govern ourselves with our higher functions.”
(5) Hypochondriacal obsessions. Janet put into this category preoccupations with the possibility of death through sickness or accident, preoccupations with suffering related to sickness or injury to the body. Obsessively hypochondriacal individuals look upon sickness and death as a cessation of the joy of living. To prove this Janet cites the typical phrase of such patients: “Everything is senseless, worthless, because it all will be destroyed by death.”
I think that these symptoms which Janet evaluates as pathological expression of obsessive psychoneurosis represent the highest existential and moral attitude that one can reach (cf. “Obsession of death,” p. 144). It is true that certain forms of neurosis appear to have pathological symptoms, but in general, the most important directions in psychoneurotic processes are those of concern for the world around and of search in the world within. I have the firm conviction that we need to study neurosis from
152
the developmental point of view rather than the statistical one in order to better understand the meaning of these phenomena. I am also convinced that the long established practice of referring to a statistically established norm surely has induced inappropriate forms of development among scores of unknown “sick” individuals by persuading them of their inferiority, illness, by concentrating exclusively on the negative aspects of their difficulties. Yet no statistical research has been done to establish positive or negative correlations between different forms of psychoneurosis and positive personality traits. The developmental, creative and superior value of psychoneurotic symptoms has not yet been given proper attention in scientific investigation of human behavior and development.
I remember a story which took place in Wilno (Poland) during the Russian occupation while misery raged in the city. A certain rich man used to ride in his carriage and distribute large sums of money to the poor. After a while the authorities put him under arrest and placed him in a mental institution. It was clear to the officials that such behavior meant anarchy or madness. Very often we do likewise when we look upon crimes as normal events in life, but great empathy, great refinement, and positive aspects of strange behavior cause in us astonishment if not opposition.
6. The Therapy of Psych neurotic Obsessions
The treatment of obsessions is the same as for other forms of psychoneurosis (Chapter 13). There must be a detailed diagnosis which offers an objective and multidimensional examination of the patient’s creative abilities, his originality and authenticity. Only then can one hope to convince the patient point after point that he possesses close linkages between certain “pathological” symptoms and the particular forms of his developmental potential and his mental richness (altruistic and existential anxieties, depressions and self-criticism, obsessions, insight, feeling of responsibility). The diagnosis must be concrete and extensive; it must have the power of a documented evidence of the value of psychoneurotic processes in mental growth. Practical conclusions must relate accurately to the patient’s life situation.
To sum up, the therapy must help the patient to recognize the positive value of his condition.
153
CHAPTER IX
PSYCHONEUROSES AND MENTAL DISORDERS
1. Definition of Psychoneuroses
In our opinion most Psychoneuroses are cases of very high hereditary potential for development. Psychoneuroses are forms of accelerated mental development which occurs through the process of positive disintegration. This process entails internal and external conflicts while building a hierarchical inner psychic milieu. The environmental factors and the autonomous factors (conscious self-determination) play a very great—but not equal—role here. The environmental factors play a greater role when the autonomous factors (and, therefore, the developmental potential) are not very strong. When the autonomous factors are strong the influence of the environment is of lesser importance (see Chapter 6, Section 1).
2. Psychoneuroses and Psychopathy
In the context of the theory of positive disintegration, psychopathy represents a primitive instinctual structure. Intelligence is subjugated to this structure and plays a purely instrumental role. A psychopath is one whose personality structure is strongly integrated at a low level. He has a low sensitivity to the attitudes and feelings of other individuals; he has very strong egocentric dynamisms; he is indifferent with regard to everything outside of his narrow interests. He is a “strong” person. He does not experience any disquietude with himself, such as is common among psychoneurotics; his inner self appears to be free from conflicts. In other words, he is not subject to multilevel disintegration.
A psychopath is also little susceptible to unilevel disintegra-
154
tion. Able individuals who rave high ambitions and a psychopathic psychological makeup corresponding to the upper range of primitively integrated structures (i.e. near the borderline of level I and level II) may, in consequence of very grave experiences and usually in the second half of their life (between the age of 40 and 60), be subject to unilevel disintegration. In such a case their breakdown takes the form of a paranoidal disorder, or distinct paranoia. This breakdown of the primitive structure constitutes some, although limited, advance of their individual development.
The psychopath is incapable of a critical attitude with regard to himself. He may appear to have a “strong will” which is an expression of an ambition united with very strong basic drives, and intelligence (often highly developed) serving as their tool. He may appear to have “self-control,” but it is geared to his egocentric plans of operation and methods of carrying them out. There is an “enthusiasm” in enjoying the power of realizing his plans. Obviously it has nothing in common with self-control based on empathy and understanding of others. Psychopathic individuals are ruthless and aggressive in subjugating every-thing to their own designs. This is their strength and their weakness. It is, an expression of a primitive “strong will” and not of a “free will.” The psychopath has no empathy only syntony in regard to those with whom he is associated by temporary ties of common venture, partnership or business. Without disintegration, without sensitivity, without internal conflicts there is no possibility of developing even a medium level of syntony (i.e. having feelings common with others). He is never aware of a common endeavor as expressed by “we”; instead his constant reference is to the “I.” He may identify others with himself but never himself with others. Psychopaths are emotionally cold, their adaptation to the environment is based on the needs to satisfy their basic drives, something that is not hard to rationalize. Because of this, the psychopath is asocial and can become antisocial.
The psychoneurotic individual is totally different from the psychopath. The psychoneurotic individual is sensitive, anxious, and has a facility for transposing psychic processes onto the autonomic nervous system. The autonomic nervous system stays in close relationship to emotional experiences. Hence
155
emotional tensions are picked up by the autonomic system and expressed as psychosomatic disorders. The psychoneurotic exhibits hyper-sensitivity, often dissatisfaction with himself, feelings of inferiority with respect to himself and to others, and feelings of guilt. He develops an objective attitude toward himself but subjective and individualistic toward others. In his inner psychic milieu he develops an increased self-awareness and introvertive knowledge of himself which gives him a key to his multilevel personality structure. It is a process of self-experience, that is to say, he realizes the multilevelness in his own structures and functions. This sensitivity, susceptibility to psychosomatization, to anxieties, plus the nuclei of the inner psychic milieu, are the substratum of disintegration and accelerated development. That is why he represents a personality capable of disintegration and capable of definite and often accelerated development. The psychoneurotic shows a tendency for conflicts in the external environment, but even more so, within his own inner psychic milieu. In contrast to a psychopath, who causes suffering in others through external conflicts, the psychoneurotic suffers along and lives with his conflicts by himself.
As opposed to the psychopath, the psychoneurotic has strong self-awareness. Any process of disintegration, but especially psychosomatic disorders, multilevel disintegration and internal conflicts, create the conditions by which self-awareness begins to grow.
As we have mentioned, mental dynamisms in a psychopath are integrated at a low level, while the psychoneurotic is capable of disintegration at medium and high levels of functions. The essence of a psychopathic structure is the cohesive union of strong primitive drives. At a low level of primitive integration (i.e. far below the borderline of unilevel disintegration) the psychopath does not have any distinct possibilities of loosening or breaking down this strongly integrated structure. A positive development in a psychopath is possible only if he has in his structure some psychoneurotic traits. The psychoneurotic, on the other hand, is capable of continual development through the process of disintegration, which often enough continues in the direction of secondary integration.
156
The disposing and directing center in a psychopath is identical with the strongest drive, or as is more often the case, with an integrated group of strong drives. Intelligence and intellectual activity are subordinated to these drives and although thinking, is rationally “correct” it is still delineated by them.
Psychopathic aims are based on strong primitive drives (ambition, pride, security, power, need to dominate) which in conjunction with a narrow and rigid mental structure gain in unidirectionality and ruthlessness since they are not controlled by empathy, responsibility or the process “subject-object in oneself.” An intelligent psychopath is at times capable of changing the direction and methods of his behaviour, but that is done only in the service of his egocentric goals.
Among neurotic individuals, the disposing and directing center presents quite a different picture. Because of the characteristic process of disintegration, especially multilevel disintegration, the disposing and directing center in psychoneurotics has no stable position. In some periods it may be established a, a low level of functions or it may move to an intermediate level (see Chapter 7, Section 1). Finally, in a period of strong development of personality and its ideal—it is localized at a high level.
During the stage of unilevel disintegration, psychoneurotics may exhibit several such centers as well as changes in their localization. For example during maturation we can observe changes from feelings of inferiority to those of superiority. This means that the psychoneurotic individual is prone to ambivalent tendencies and to changes in evaluation and judgment.
The instability of the disposing and directing center in psychoneurotics and its definite localization at a low level in psychopathy is related to the structure of the inner psychic milieu. In fact it is difficult to talk of the inner psychic milieu in a psychopath, since his self-awareness is very primitive. Because his functions are too tightly integrated they lack segments (functions or processes) which could be more or less autonomous and thereby free to cooperate or to oppose each other. Because of this one can say that the psychopath has a very low level of self-awareness or, perhaps,
157
none at all. All of his mental activity is controlled by instinctive dynamisms at a low level.
The psychopath—although not subject to any multilevel disintegration—may experience feelings of inferiority. However, this is with respect to the external environment—never with respect to the self or to his own unfulfilled possibilities. The psychopath has no nuclei of universal development, he has no nuclei of the inner psychic milieu, no conscious concern for the course of his personal development so that his process of valuation is not internally gauged (absence of the third factor). Lacking a universal model of his development he fellows a narrow structural model of egocentric ambition. His ambitions have no relation to empathy, essence, and personality (see Chapter 10, Section 1). Psychoneurotics, on the contrary, are very much aware of their unfulfilled developmental possibilities. They perceive personality as a model (in the sense of the concept defined in Chapter 10, Section 1); as a consequence of their need to realize this model they experience tension; they have an awareness of developing their inner psychic milieu, which gives them a sense of their ideal and of new possibilities of growth.
General weakness, emotional fatigue, loss of proper psychic tonus may periodically appear as signs of lack of growth, stagnation, or even temporary descent to a more integrated lower level, as a way of handling tensions otherwise too extreme to absorb. However, a continuous insight into the inner psychic milieu (which is characteristic of the process of disintegration), disquietude, dissatisfaction with oneself, feelings of guilt and sin, feelings of inferiority with respect to oneself-all of which are in a sense sources of inner tension—most often tend to lead psychoneurotic individuals to a higher level of disintegration and integration.
All the above processes are absent among psychopaths.
The dynamic factors of a psychoneurotic personality structure are: the formation of the inner psychic milieu, realization of the hierarchy of values within oneself, and a strong tendency for growing in the direction of ever higher values up to the personality ideal. Concomitant with an increase in
158
awareness and clearness in visualization of the personality ideal, an individual is increasingly conscious of his distance from it. The appreciation of its value, the reality of this ideal—and the power necessary to reach it—continually gain precision and clarity. The disposing and directing center being close in its dynamic localization to the personality ideal takes from it strength and transmutes it into dynamisms working methodically and concretely on restructuring personality. This is the principle of inner psychic transformation. Many individuals at this level of development speak of the ideal as a continuous source of strength.
Nervousness and psychoneuroses are structural conditions of sensitivity within and towards one’s own inner psychic milieu wherein positive development through unilevel and multilevel disintegration finds especially favourable ground. Without these processes the author does not see much possibility of positive development of human personality. Without nervousness and neuroses there is no positive disintegration, and without positive disintegration there seems to be no positive development.
Let us now go on to discuss the relation of psychoneuroses and psychopathy to human creativity. A psychopath, as a rule, does not create any work of genuine cultural significance. His intelligence, even though it may be very high, is never truly creative. That is why even a very extensive use of intelligence by a psychopath does not lead to creative ideas and activity, but rather to destructive activity.
The “creativity” of outstanding psychopaths is not controlled morally, has no empathy, but instead is an expression of striving for the realization of narrow and rigid goals under an enormous tension of egocentric ambition. Lack of empathy, universality and responsibility prevent psychopathic achievements from being considered as genuine and authentic creativity. Some activities of psychopaths may appear in the initial stages to be creative, but in essence, and after longer periods of observation, it becomes clear that such activity is destructive (for example Hitler’s path to greatness for Germany).
It is because of the strong instinctive dynamisms that it is difficult for a psychopathic individual to evaluate and to measure either his own or other people’s activity with respect
159
to any future perspective. It stems from the lack of inhibition of his egocentrism by empathy (or love), lack of responsibility and lack of any “hierarchical” awareness. That is one reason why he has no ability for entering into the mental and emotion states of others and is not able to recognize the value social, moral and cultural problems and issues.
Not so with psychoneurotics. They are capable of producing works of cultural importance not only because of their high intelligence, but also because of their sensitivity, capacity f introspection, ability for self-criticism and critical evaluation of others, ability to discern a variety of levels in values and to have the experience of “subject-object in oneself.” This due to their high susceptibility to processes of positive disintegration, as a result of which they acquire a high capacity for “objectivity” when dealing with themselves. And for “subjectivity” when dealing with others through a high level empathy (see Chapter 10).
3. Psychoneuroses and Psychoses
Nervousness, neuroses, and especially psychoneuroses, bring the nervous system to a state of greater sensitivity. They make a person more susceptible to positive change. The high psychic structures gradually gain control over the low ones. The lower psychic structures undergo a refinement this process of inner psychic transformation. This transformation is the fruition of the developmental potential which makes these states possible and makes possible their further development. The components of the development potential like enhanced overexcitability, nuclei of the inn psychic milieu, and special abilities and talents play here an active role. Through multilevel disintegration there occurs positive evolution, making possible the achievement of a high level.
How does this apply in the case of psychosis? We take the position that in psychoneuroses the highest neuropsychic centers are active and provide a decisive source of psychotherapeutic and developmental energies. They are the sources which energize the developmental process away from integration at a low level. Through the “pathological” changes of psychoneuroses, to inte-
160
gration at a higher level. In psychoses, however, the higher neuropsychic centres are often damaged, which is the cause of a much greater probability of pathological involutionary disintegration. In many cases of schizophrenia where we encounter symptoms of involution and dissolution we can postulate organic malfunction especially that the malfunction is observed first in the sphere of complex higher activities without initially attacking lower functions. Supporting evidence for this view comes from prefrontal lobotomies which separate higher cortical levels of activity (by elimination) from lower subcortical ones which go on efficiently, perhaps even better because of disinhibition.
What, then, are the main differences between psychoneurosis and psychosis, especially schizophrenia?
In both processes, symptoms of fears and obsessions may be common; in both we observe strangeness of behaviour, weakening of the reality function and inability for adaptation to changing conditions of life. In both groups of syndromes social contacts are either disturbed or reduced or there is a tendency towards isolation and self-mortification; there occurs a more or less pronounced loosening between cortical and subcortical centres and their respective activity. Cortical activities may be carried out on a high level but from time to time there may occur a “descent” to the level of subcortical activity expressed by outbursts of egocentrism or even aggression. Tics and other signs of automatism of movement may appear such as excessive wandering “without purpose,” facial grimaces, spasms or twitches, which express either incomprehensible or actually very clearly understandable emotions. There may be a temporary weakness or total absence of the function of the will (hypobulia and abulia) expressing a weakness or incapacity to act. This may not encompass all levels of functions but only some. Reduction of the function of volition is the concomitant of a deep depression.
What, then, are the essential differences? One of the most basic differences is the fact that there are no stable intellectual disorders in psychoneurosis. The psychoneurotic has no essential disorders in association of ideas, and is able to see the connection between cause and effect; he is subject to no
161
delusions. His own strange behaviour produces, as a rule, self-correcting mechanisms. Such an individual occasionally exhibits a sense of humor, is able—periodically—to rid himself of some automatisms. He may shake himself out of his inactivity and withdrawal, break out of his depression or sadness in order to give himself to empathy and a concern for others. This is an expression of the process “subject-object in oneself.” He does not, therefore, lose control and direction of himself does not completely break his contact with reality, and uses his reality function while it is periodically weak. Furthermore, psychoneurotic syndromes are not related to any substantial mental handicaps. Psychoneurotics, and especially those at a higher level of development, do not give evidence of a lasting mental impairment. They may have certain halts, disproportions or delays in their development which, however, do not last but are related to compensatory or sublimatory “developmental leaps” of the functions arrested in development, but there is no essential intellectual regression.
In lighter cases of psychoneurosis we find tendencies to regress to the childhood period without, however, being subject to the more or less automatic processes of negative regression. Negative regression may appear either in lighter cases of functional disorders, as in lower forms of psychoneuroses, or in educational difficulties, or in severe psychotic and organic disorders. An increasingly chronic state of hypochondria would indicate negative regression. A growing egocentrism leading to outright egoism and loss of empathy and understanding of others would also indicate negative regression. Other examples of negative regression are instances of uncontrolled obsessions of jealousy which make a person blind to any evidence to the contrary; or in psychoses, a chronic descent to the level of “aggressive autism,” defensive isolation, contracted postures, etc. Only in rare cases psychoneuroses make development difficult. In the vast majority they are a necessary concomitant of positive, and even accelerated development.
Psychosis is more often characterized by a process of involution. It is not merely the loosening and disintegration of structures without injury to basic psychic structures but rather the dissolution of the structures themselves, the result being
162
an emotional flatness, irreversible regression of intellectual and emotional functions, or loss of the reality function. An arrest in one area of functional development in a psychoneurotic is usually compensated by the positive growth of other functions; in a psychotic, however, very often we detect no development at all. To give an example, a young woman, 26 years old, was suffering from a severe depression combined with a loss of ability to act (abulia). When she learned that her very close friend was gravely ill she came out of her depressed inactive state, traveled to another city to stay with her friend and took care of her. After returning home she became depressed again but not as severely as before. This shows a compensation of feelings, and also a sublimation of feelings expressed in the temporary activation of her emotions on the highest level (altruistic concern for another person).
Such compensatory reactions are found in psychotics less frequently than in psychoneurotics.
Psychoneuroses—in the author’s opinion—are most often an evolutionary process in a positive sense (i.e. there is growth), which in rare instances of some very difficult and unfortunate cases however, may turn to involution. Psychosis, on the other hand, is in the majority of cases an involutionary process, and only under certain fortunate conditions of the environment (or of inner psychic milieu) may it have a positive outcome. The psychoneurotic does not regress to a lower level; the psychotic on the other hand is characterized by a more or less rapid process of intellectual and affective deterioration. Of course, it is conceivable that a psychotic process may initiate an upward growth to a higher level than before the psychosis. Cases of such remissions are known, although they are not common. Clifford Beers was one of such cases. His most intense personality growth and his activity in initiating the movement of mental hygiene occurred after his psychotic period. Jack Ferguson was another such case in whom the paranoidal structure disintegrated and came under the control of his great empathy and his social and scientific conception of a new psychiatric approach toward patients. Both cases have been described elsewhere (Dąbrowski, 1967b.).
This means that we can find processes of positive develop-
163
ment in psychoses. In such cases the kind and the strength of the developmental potential outweighs drastically the involutional processes. As a consequence of reaching a critical stage of development, and of particular constellation of external circumstances, comes a creative burst of positive forces—frequently as a tragic internal battle—bringing about the transformation of the psychotic process into accelerated development. Nevertheless such cases are relatively infrequent.
Let us make clear the differentiation between psychoses—in particular schizophrenia—and psychoneurosis. It is important to distinguish chronic forms of schizophrenia from acute, although this does not yet bridge the gap between the acute form of schizophrenia and psychoneurosis. There is an important difference between structures and functions of a schizophrenic process and a psychoneurotic process. It is true that an acute schizophrenic process is positive in its course and resolution more often than the chronic process. Frequently, as described above, the acute form is an expression of a conflicting pressure of mixed forces (negative-positive) which are too powerful for the individual to handle and sort out. But even some chronic forms, especially those on the borderline of schizophrenia and psychoneurosis, may have a positive outcome.
Both the acute and the chronic processes often contain ambivalences and ambitendencies, distinct though partial hierarchizations of values, loss of volition or high tension of psychomotoric activity (also aggressiveness), motionless postures or offensive behaviour.
Older youths and adults have in addition hallucinations and delusions. Not infrequently certain complexes of symptoms of “internal hell,” fears, obsessions, depressions, suspicions, resemble the states pictured in “Bardo Thodol”—the Tibetan Book of the Dead describing the after-death states and final judgment. The symptoms may resemble drug “trips.” They occur usually before a new phase of development.
The types of schizophrenia: simplex (slowly developing, often for many years) paranoid, catatonic, and hebephrenic, are not sufficiently differentiated in respect to their etiology, pathogenesis, and prognosis. It is generally assumed that the least differentiated and most often developing on the basis of changes
164
in brain tissue is schizophrenia simplex, while catatonia is regarded as developmentally most promising. Each form of schizophrenia has some kind of psychic overexcitability or a mixture of several kinds.
To make our discussion clearer we shall now examine two clinical oases.
Case 12.
S.J. was a 6-year-old boy who was received on the children’s neuropsychiatric ward of the Institute of Mental Hygiene in Warsaw in 1951. His behaviour was marked by fear: when someone was approaching him he moved away, he would not allow to be taken out of the room, or would suddenly run away from the room. Like other children he would repeatedly demand to be taken to games and playground activities, yet when someone wanted to take him there he would back away, or would resist attempts of taking him out of the room. His face and eyes usually expressed fear or anxious alertness. He played with toys or things given him but did not care to keep them. When playing with a ball his pitches were always fearful. He understood simple orders and sometimes would carry them out at once, at other times would show no response but would later carry out the order without being reminded. He had periods when he would say almost nothing and remain without contact with his environment. At other periods he talked a lot, approached other boys and tried to get them involved in the games he set up. For a long time he was an inseparable companion of an older 16-year-old boy who was entirely passive towards his affections or aggressions. S.J. laughed at him and sometimes imitated every one of his movements.
In relation to adults S.J. was on several occasions aggressive when he kicked, beat, and spat. Often he would jump from his place and without a word throw himself on an adult and hang on him with his whole weight. It was hard to get him away since he was able to take all kinds of postures by bending in all directions with an astonishing ease.
He liked music very much (radio) and constantly called for
165
the book of first grade reading which he called Ala-As (Ala was the name of a girl in the book and As was the name of a dog). During one week he was constantly asleep and would fall asleep even at meals and slide to the floor. In the weeks preceding the present examination he showed unusual appetite, so that he would throw himself on the food bowls of other children, eat whatever he could and then returned to his own bowl which he left at his place. It was difficult to watch him because his movements were extremely quick, and because he would not react when called but instead would look at the bowl he set his eyes on as if in a trance.
These symptoms are psychotic with a strong indication of organic changes in the brain. At an earlier age when his teeth were cutting he had high fever. Most of the infectious diseases of childhood he had in a severe form, and after the operation of his third tonsil he could not speak for several months.
Neurological examination showed an unstable Babinski on the right side, Chwostek on both sides, and enhanced red dermorgaphia.
Together with the described symptoms we observe a high degree of impulsive behaviour, high degree of fatigability, sleepiness, which indicates a neurosomatic disequilibrium. The boy shows fear, autism, and total lack of control normal for his age. He manifests enhanced psychomotor excitability, also sensual and primitive affective overexcitability.
Case 13.
J.G. was a 10-year-old girl accepted on the same ward in 1946. Her movements were slow, and gave an impression of certain artificiality, as if she were walking on stage. During physical exercises she would often not practice with the group but move aside or even in the midst of others and then would suddenly start bending and moving like a ballet dancer.
When asked a question she would sometimes answer but more often it would seem that she did not hear the question. J.G. gave the general impression of being in a waking dream. She talked to herself as if someone else was talking to her: “Julie, don’t be afraid of the doctor,” or when she came for
166
her shots: “Julie, don’t cry, don’t scream, Julie,” and saying this her face would move as if ready to cry.
It was observed that she was inclined to repeat the same action a great number of times; for instance, she would button and unbutton for a quarter of an hour, or longer, the coat of someone whom she accidentally met. She was destructive. She would tear books, toys, pictures and seemed to do it with great satisfaction. On other occasions she would look at pictures and books for long periods of time giving the impression that this occupation was providing her with stimuli and brought to life her world of imagination. On such occasions her movements were harmonious and the expression on her face showed subtlety. She also showed tendencies to tease other children displaying in it a lot of detached interest.
J.G, has undergone fever and shock treatment without any results.
The symptoms of this case indicate schizophrenia simplex or to some extent hebephrenia. The child showed these symptoms for several years in a number of different ways but always characteristic of severe psychic disorders. There are components of increased excitability of her imagination.
Both these cases are examples of involutional disintegration. There is every indication of irreversible brain damage.
4. Schizoneurosis
Let us add a few summary remarks with respect to a dynamic differential diagnosis between psychoneurosis and psychosis, using as a vehicle of comparison, schizoneurosis, introduced by Paul Abély to indicate the borderline state between psychoneurosis and psychosis.
Schizoneurosis is a clinical entity which in respect to its etiology and pathogenesis is a transition form between psychoneurosis and schizophrenia. Schizoneurosis was first described by Abély (Abély and Delaville, 1960). A brief description of schizoneurosis will allow us to define the critical points of diagnosis of the two classes of syndromes and to characterize possible ways of preventing schizoneurosis. Positive and subtle influence on the development of empathy, control and respon-
167
sibility in grave cases of psychoneuroses activates elements which prevent the development of schizoneurosis.
In respect to psychoneurosis schizoneurosis is an analog of the decompensation of heart action. In schizoneurosis preventive forces grow weak and deformed. There is a gradual loss of self-control, of contact with the environment, of prospective abilities, of intellectual activity and affect. What remains are certain preventive forces of somewhat automatic nature and remnants of a reduced reality function together with some elements of irony and humor which resemble vaguely something of the dynamism “subject object in oneself.” Reality function grows weak. Sensory perceptions are strong but appear fixated to narrow and rigid areas (Dąbrowski, 1967a).
The following case gives a clinical picture of schizoneurosis.
Case 14.
M.W. was a young man 22 years old. There was no history of mental disorders in his family. His mother was a refined person, rather calm and deeply loving her son. His father, deceased several years back, was described as a domineering, although not extremely, authoritarian person. M.W. displayed enhanced excitability of imagination and intellect already at the age of 3 and 4 [cf. Chapter l, Section 6 (1) b]. He was always introverted. His period of puberty was more difficult than normally observed. At that time he showed strong ambivalence and contradictory tendencies in behavior, he disliked his father, and would leave home for many hours without telling anyone. He was autistic, obstinate, and manifested low degree of contact with everyday reality. In spite of these difficulties and additional ones in his school work he graduated from high school.
After graduation his autistic behavior increased. He would disappear from home for many days and spend nights either with some friends or, if it was summer and the weather was nice, somewhere in the country. He spoke little, sometimes did not answer his mother’s questions. He had his own peculiar sense of humor, for instance, when his mother once asked him where he went he said: “Here and elsewhere, but mostly elsewhere.”
168
He went through periods of entirely sleepless nights and often he would spend the entire night walking outdoors.
He would not allow to be examined neurologically. A superficial examination revealed increased excitation and inhibition of muscular reflexes, positive Chwostek, extended and enhanced red dermographia and pronounced waxy flexibility.
For many years his condition remained the same without change for the worse. His contact with me as his psychiatrist was good, though irregular.
Prognosis in a case like this is uncertain.
We believe that psychic tension, anxiety states, aggressiveness, etc., in psychoneuroses are not isolated conditions, but are strictly related to the whole personality of the individual and exert a positive developmental influence. Aggressive attitudes are more often an expression of strong inhibitions and inner difficulties in the realization of basic drives and needs, rather than of blind, unconscious forces. For instance, emotional outbursts result occasionally as a function of a very strong sensitivity and subtlety remaining under great pressure of accumulating “internal protest” against the brutality of everyday life. Conditions of anxiety or dread are often connected with the difficulties of changing oneself while one moves from a lower to a higher level through the process of positive disintegration (see Chapter 6, Section 8 describing a state of “suspension” between levels). This happens, for instance, when a person experiences at times resistances impossible to over-come in dealing with his problems and at the game time feels rather deeply the reproaches, demands, and even aggressiveness on the part of his environment.
In psychoneurotic anxiety we often find disquietude and dissatisfaction with oneself, feelings of guilt, and depression. Neurotics are often prone to anxiety states and an excessive desire to explain their own condition: they have an excessively “educated” consciousness. These attitudes are absent in schizoneuroses, or are expressed nonverbally by a silently angry or stiff face when the doctor or nurse fail to notice them while talking to another patient. There are no definite developmental needs; defensive forces do not represent basically creative
169
traits, but rather are rigid. We find here a breakdown and partial disintegration of motives, weakening of the ability to understand one’s own anxiety, and aggressivity. In case 14, M.W., we see that in certain periods there was total lack of motivation in his behaviour, very strong autism, incongruency of facial expression and his behaviour which was often unpleasant to his family and others. These instances indicate lack of control of himself and of contact with others, resulting in bouts of insomnia and possible hallucinations.
We can also say that, in the great majority of cases of psychoneuroses, we are dealing not only with strictly defensive forces, but—as we have indicated—with developmental powers (creative interests, search for insight, need of changing oneself, etc.), while in schizoneuroses we have only some remnants of weak, deviated defensive forces, and developmental forces are deteriorated or even destroyed. The defensive forces operate automatically on restricted areas, for instance, as a tendency to remain in isolation, to stay motionless, or to sleep, or to spend all the time with one isolated interest. Power of control, emotional projection, and intellectual activity fall apart.
It is also characteristic of schizoneuroses that there results weakening and loss of the reality function with respect to daily needs and occupations, without, however, any compensation at a higher level. Response in the area of emotions and imagination is intense, but fixated unequally to narrow areas of life, while the ability for inner transformation is deeply shaken or eliminated.
Let us now throw some light on the differences between structures and dynamisms of psychoneuroses and schizoneuroses based on results obtained by Z. Piotrowski (1957) using the Rorschach technique, and also some additional findings.
The results of these investigations may be summarized as follows:
a. The presence of psychoneuroses is indicated in the Rorschach by the fairly clear and active, cooperative human, kinaesthesis. Furthermore, there are no intellectual perseverations; there is a high percentage of clearly perceived forms, in all their variety, a considerable number of color responses, a fair degree of high quality, constructive, global responses.
170
In schizophrenia and schizoneuroses the above picture is usually reversed.
b. If the adjustment to reality appears poor, and at the same time strong anxiety states are present, this indicates schizophrenia or schizoneurosis.
c. Strong anxiety response in the Rorschach with retained self-observation and self-control indicate psychoneurosis: with a loss of self-control they point to schizoneurosis.
d. The more the clinical picture resembles changes characteristic of organic cortical changes, the more we can suspect schizoneurosis or schizophrenia.
e. Apathy, lack of imagination, regression to the world of dead and immobile objects, lack of color and human kinaesthesis, a limited number of well observed forms—all indicate schizoneurosis, without many psychotherapeutic possibilities.
According to Greenblatt and Solomon (1953)—if disorganization affects emotional functions then the prognosis is fair, or even good; if there is lack of emotional tensions, and the disorganization affects mainly cognitive functions the prognosis is doubtful or poor. When emotions grow weak then the motivating power in life also grows weak, while intelligence which is its instrument now left to itself degenerates.
We would like to know the causes which determine that some neuroses succumb to structural decompensation, and pass into schizoneurosis or schizophrenia, while others have a positive outcome. There is yet no background of biochemical, neurological, psychological and psychiatric research or investigation adequate to answer this question. On the basis of the theory of positive disintegration we may outline some opinions only, which, depending on further experience and investigation, require either verification or rejection.
In our view, those neuroses or psychoneuroses succumb to decompensation, or structural impairment, which exhibit the following:
1. A hereditary endowment with only one-sided form of the developmental potential, e.g. special skills or abilities which pertain to one activity only but are not combined with different kinds of emotional overexcitability or a wide range
171
of interests, for instance a special talent for playing chess, a keen memory for facts and dates but not for deeper understanding of history, a sharp intelligence for an objective quantitative research career in science but lacking the ability to put the interpretation of the findings in a wider context, or even to see its philosophical implications. Consequently adaptation to a hierarchical conception of reality and values (multilevel disintegration) is poor, being not global but narrow. Inner psychic transformation and self-control are also weak, while there may be some creative ability, however the sensitivity to internal and external stimuli is very high.
2. Disproportion between excessive and irregular tension of blind defensive forces and the concomitant weak developmental forces and intellectual endowment. The forces of defense against disequilibrium act blindly “not knowing whom to serve,” the defensive response is more or less automatic, restricted to narrow areas, out of contact with the forces of development which are weak and, therefore, cannot provide direction. The defensive tendencies often react in the form of panic which does not allow broad and conscious action.
3. A medium strength of the developmental potential and an excessive number in the personal case history of grave experiences.
4. Possible organic changes in the cortical tissue usually difficult to pinpoint, but which block a full realization of the developmental potential. In many cases of schizophrenia and related conditions there is a history of severe infectious diseases, high fevers with signs of subsequent neuronal disorders, and also rapidly advancing states of apathy, loss of reality function, dissociation (e.g. Cases 12 and 13).
5. Psychoneurosis, Paranoia, and Paranoid-like Conditions. The problem of differentiation between psychoneurosis, paranoia, and paranoid-like conditions is so special that we think it worthwhile to treat it separately.
172
In our view, paranoia—in common with other psychotic forms of a schizophrenic character—is a pathological process. Paranoia is fairly closely related to psychopathy.
Paranoid schizophrenia is a process while psychopathy is a structure. Paranoid schizophrenia shows internal stress, internal conflicts and an. Inner psychic milieu. These are absent in psychopathy and paranoia.
In spite of the fact that in paranoid schizophrenia we have certain forms of pathological integration such as the “directing nucleus” of delusions and suspicions, nevertheless there is an essential difference between paranoid schizophrenia on the one hand, and psychopathy and paranoia on the other. In paranoid schizophrenia the directing nucleus is subject to, variations, or even processes of disintegration; also paranoid schizophrenics are often responsive if a suitable approach is used. Their whole structure is subject to fluctuations alternating between the positive and the negative direction. It is thanks. To these traits of instability of the schizophrenic structure that we have cases of remission and return to health. Under the influence of a constellation of internal and external stimuli there may occur a “developmental leap” by which a positive and integrated disposing and directing center is formed at a higher level. This, however, does not happen very often.
One needs to add that the tendencies to suspicion or aggression in paranoid schizophrenics do roc stem from integrated primitive drives as is the case of psychopaths, but rather from chaotic uncontrolled emotional tensions.
“Great” psychopaths in the moment of their ultimate defeat show the breakdown of their rigid psychic structure. There is no positive transformation but transition into the process of paranoia characterized by unfounded suspicions, reactions of cruelty, delusions of persecution, or of grandeur.
It is not uncommon—in my opinion—that psychopathy is, connected with the paranoidal process in those cases when very strong structural and functional patterns in psychopathy are such that there is high tension due to specific environmental conditions, particularly if the psychopath encountered especially difficult circumstances which have limited his most important
173
aims and drives. For instance irritable individuals endowed with very strong ambition and egocentric psychic tension when met with failure may undergo a negative psychic breakdown manifested as suspicions and delusions (e.g. Stalin). Paranoia is characterized by delusions of grandeur, by delusions of persecution, by feelings of superiority, which are expressive of strong inner dynamics, on the one hand, and, on the other hand, of suspiciousness; expressed in the conviction that the environment has been organized to paralyze, fight, and destroy the paranoiac’s personal interests. It reflects, on one hand, a special type of pathological integration of high tension guided by a delusional center, and on the other hand, destruction of all previously existing contacts with the people in his environment.
A paranoid individual has no counteracting mental forces within himself, such as the prophylactic powers of the inner psychic milieu, simply because this milieu has never been developed. This is not true of lighter forms of paranoid schizophrenia and severe psychoneurotic obsession, where the dynamic elements of the inner psychic milieu can at times be discerned fairly clearly.
A strongly paranoid person has no corrective powers (no feedback receptors) with respect to his own behavior. He is given to action and reaction without participation of the inner psychic milieu, for which is substituted a delusional nucleus, of persecution, or of greatness, and mobilizes “defensive” dynamism against “danger” from without. In consequence he may equip his house for safety to an excessive degree. Great paranoiac psychopaths change suddenly their bodyguards or the whole security force, and react on the least suspicion with persecution, aggression, and cruelty. Many such individuals may be described by what the French call “persecuted persecutor.”
Can we speak of the disposing and directing center in paranoid individuals? I believe we can. This center is represented by the delusional nucleus, that is to say, strongly coupled delusions and aggression at a lower level. Except for this delusional quality, such a center is similar in character to the disposing and directing center of psychopaths.
174
As we see, the paranoid structure differs essentially from the structure characteristic for psychoneurotics. The main difference is represented by the presence—in the latter case—of a well developed inner psychic milieu with the presence of the third factor, and a capacity for inner psychic transformation, all active in the process of positive disintegration.
A paranoid individual does not manifest, therefore, any astonishment dynamism, nor disquietude with respect to himself, nor feelings of some dissatisfaction, shame or guilt, feelings of inferiority with respect to himself, nor the dynamism “subject-object in oneself.” There are no indications of the third factor, which would make it possible to establish practical judgment in accepting some and rejecting other elements, that is, establish a genuine, positive or negative attitude towards the environment. Such an individual does not manifest self-control or inner psychic transformation. Self-control and inner psychic transformation are possible only when there are operating strong multidimensional hierarchical forces, such as differentiation of a “higher” and “lower” self, the differentiation of the subject and the object within oneself, and the differentiation of developmentally positive and negative choices (the third factor). In rare cases paranoid individuals develop these dynamisms and recover, as was the case with Jack Ferguson (Dąbrowski, 1967).
Paranoid individuals in general are not subject to the process of positive disintegration. They are integrated at a low level and do not exhibit inner conflicts, but show, rather, a tendency to aggressiveness, external conflicts, and anxiety states with respect to the environment.
Such individuals do not exhibit, which is logical, either any coupling or dynamic relatedness between their external and internal responses, which is the very basis of the process of inner psychic transformation. In the absence of a hierarchical inner psychic milieu and of multilevel dynamism such as “subject-object in oneself” and the third factor, a process of refashioning oneself is not possible, on the contrary, it is the external world that is refashioned by means of suspicions, delusions, aggressiveness, even crime. We have mentioned that in less severe cases of paranoid schizophrenia we are dealing
175
with temporarily present, deformed and hardly conscious dynamism of an inner psychic milieu which can even be hierarchical.
With respect to such individuals, an early enough diagnosis (already at the age of 5 or 6, or during adolescence) of a lack of inner psychic milieu, rigidity of structures and functions, and, on the other hand, the presence of sensitivity and feelings of inferiority and superiority with respect to the external milieu, is the only basis for a program of prophylactic activity. A very cautious and slow development of sensitivity with respect to oneself (building up of nuclei of the inner psychic milieu), and slow inner psychic transformation, may lead—in early childhood or adolescence—to certain results in loosening, up the excessively rigid structure and diminish the perceived oppressiveness of the external environment.
6. Psychoneuroses and Mental Retardation
Definite: psychoneurotic syndromes are difficult to find among mentally retarded children. Mental retardation results from hereditary impairment, defects of innate pathological developmental patterns, birth defects (injuries at birth), impairment or inflammation of nervous tissue at childbirth. The diminution of intellectual functioning is more severe the more severe is mental retardation. It is accompanied by a diminution of the level of emotional and instinctive functions, without, however, their degeneration or deformation.
In analyzing neurotic symptoms and psychoneuroses among, mentally retarded children it is difficult to talk about psychoneuroses in the same sense that we speak of them in relation to normal children because we cannot compare them on the same level of mental activity.
One can detect some psychoneurotic syndromes in mentally retarded persons who are nearest the normal level. However, in general, a deficient mind does not deal with a rich enough material to “produce” a psychoneuroses. It, therefore, produces only deficient forms of psychoneuroses such as functional hyperkineses, tics, masturbation, short-lived and simple states of anxiety or depression. Perhaps that is why we cannot detect.
176
in retarded children traditionally recognized pathological units such as: obsession psychoneurosis, psychasthenia, hysteria, anxiety psychoneurosis, etc.
Investigation of the specially gifted children has indicated that, depending on the level of development of a child’s personality, the psychoneurosis will also have a corresponding level: of disturbed functions. This indicates that the tendency for development of a specific psychoneurosis is directly related, level by level, to the personality development in a child (see Chapter 11). This view in relation to psychoneuroses of adult individuals was expressed by Manfred Bleuler (1941) and Karl Menninger (1963; also Menninger and Menninger, 1942) (see also Chapter 7).
Our investigation indicated that the abilities, interests, and the emotions of the mentally retarded do not develop beyond a low level. They do not represent any basic predisposition towards the development of psychoneuroses.
We could observe, however, two groups of strong disorders of emotions and drives, but related to a very low level of functions. These are fear and hysterical syndromes. They are evoked by a simple external cause such as sudden appearance of a person or an object, beating, abuse, sudden fail, physical injury, noise, darkness, etc. Primitive hysterical reactions such as throwing oneself on the ground or hysterical spasms were caused by a desire to be the center of attention, to avoid punishment or some other unpleasantness.
Certain hysteroidal traits of a retarded child are expressed, among others, in variability of moods, excessive impulsiveness, or, on the contrary, through rigidity, superficiality, vanity, egoistical behaviour, susceptibility to influence by primitive suggestion, etc. It appears that excessively developed psychomotor activity—to which we shall later return—as well as some obsessive symptoms in neuromuscular areas (automatic actions), are expressive, in a primitive way, of states of primitive protest resulting from weak psychic sensitivity and absence of any control over subcortical functions. That is why the mentally retarded show much less somatic disturbance; either because of weaker transferability of psychic experiences onto the auto-
177
nomic nervous system, or due to the primitive level of these experiences, or both. Our medical investigations did not record disturbances of digestive or respiratory systems as due to unpleasant experiences. We did not detect among these children any increase of excitability or nervousness in relation to internal stimuli. Their sensitivity appeared to be developed in response to the stimuli from the external environment, which is also a characteristic trait of animal development.
Children of this kind are in continuous motion. They change their position all the time, and are under constant tension; hands and legs move about with little purpose. Among these children, hyperkinesis of facial muscles is especially pronounced producing a variety of expressions (tics, mimics, and other spurious motions). Eyes are usually very active; the tongue is often shown outside. There is a tendency for excessive showing of teeth. They move their hands up to the face for stroking or scratching. They also have a tendency for moving or clasping hands and fingers. Even when trying to be generally quiet, they always maintain an excessive excitability of certain muscular groups (leg crossing, jumpiness, movements of body trunk, etc.).
Hyperkinesis of hand, legs, and face is increased under the influence of external stimuli (noise, new situation, talk). At other times we observe the opposite effect: psychomotoric quietude under influence of external stimuli, which shows that the psychomotoric excitation and inhibition is predominantly controlled by external stimuli.
The other kind of increased psychic excitability found commonly among mentally retarded children is an increased affective activity, which does not include, however, any higher emotions. It may be expressed in outbursts of anger, joy, laughter, fear, in behavior unmotivated or very slightly motivated by emotional attachment to someone, etc. There is also a need to show off which is not tempered by even the least subtle processes of inhibition. It is also characteristic for this type of child to demonstrate before the environment all kinds of superficial feelings without participation of reflection. Minor school difficulties, incidental troubles or remarks are a cause of tears, trembling, accelerated speech, excessive hand motions, increased muscular tension, defensive movements, or sexual stimulation.
178
In these two forms of increased excitability (e.g. psychomotor and affective) among retarded children, we note the following:
1. reactions to primitive stimuli (other stimuli are not used in child’s development);
2. reactions easily noticeable externally;
3. satisfaction with primitive experiences;
4. lack in transformation of psychic excitability;
5. lack of any symptoms of increased intellectual excitability and imagination;
6. if the last is exhibited, it is only in the area of primitive, concrete, or magical thinking of an undeveloped and non-creative type.
It appears that other forms of nervousness among mentally retarded children (excessive talk, taking offense too easily, suggestibility, clinging to others, etc.) do not correspond to some totality of a well defined neurosis. Among such children these special traits may constitute a “pseudo-wealth” of a great variety of forms, i.e. mobility, restlessness, babbling, clinging, cuddling, which express demonstrativeness and “sympathy” on a very low level, but without their being joined into any coherent whole.
Depressive states are rare, and found only in those on the borderline of retardation and “normality.” Such states appear as the effect of such factors as primitive but very clear stresses like isolation from the group, etc.
Our investigations in this respect were not adequate. It would be necessary to pursue the problem of various forms of increased excitability, or nervousness, in order to discover which of those forms have a tendency to develop, or to disappear during a child’s life, depending on intellectual development and the richness of his inner psychic milieu, as contrasted with those that become rigid, being strictly connected with mental deficiency.
In conclusion we may say that among more severely mentally retarded children we cannot actually speak of psychoneuroses in the strict sense, but rather of increased excitability, both psychomotor and affective, in their primitive forms.
179
CHAPTER X
PSYCHONEUROSES AND OUTSTANDING INDIVIDUALS
Clinical work and research which gave the basis for the formulation of the theory of positive disintegration showed a great similarity in respect to the developmental potential of psychoneurotics and eminent personalities. This similarity appears to be close in regard to the course of development, its underlying overexcitability, nuclei of the inner psychic milieu, nuclei of talents and special abilities. These similarities are particularly strong when we compare the development of eminent personalities with the course of psychoneuroses at a higher level of mental functions. This problem has been discussed from a different angle elsewhere (Dąbrowski and Piechowski, 1969).
1. Definition of Personality
Personality, in the context of the theory of positive disintegration, is a name given to an individual fully developed, both with respect to the scope and level of the most essential positive human qualities; an individual in whom all the aspects form a coherent and harmonized whole, and who possesses, in a high degree, the capability for insight into his own self, his own structure, his aspirations and aims (self-awareness). It is one who has the conviction of having found his ideal, and that his aims are of essential and lasting value (self-affirmation), and who is conscious that his development is not complete and therefore he is working internally on his own improvement (education-of-oneself and self-perfection).
Personality can be described as a self-aware, self-chosen, self-affirmed, and self-determined unity of essential psychic qualities, of fundamental individual and universal “essences.” With the
180
achievement of personality these essences continue to undergo quantitative changes but not qualitative changes. These basic qualities or universal essences are: autonomy, empathy, authentism, responsibility. The individual essences (qualities) are: (a) exclusive, unique, unrepeatable relationships of love and friendship; (b) consciously realized, chosen and realized primary interests and talents; (c) self-awareness of the history of one’s own development and identification with this awareness.
Personality is thus the aim and the result of development through positive disintegration. The main agents of this development are the developmental potential, the conflicts with one’s social milieu, and the autonomous factors (especially the third factor).
Let us try to follow these related sources of development and the coupling between the two phenomena, i.e. psychoneurosis and socially and culturally recognized eminence. To do this we shall study the personality development of several eminent individuals whose life stories have also all the distinctive features of psychoneuroses. The example are as follows: Franz Kafka, Gérard de Nerval, Jan Wladyslaw Dawid, and Ludwig Wittgenstein.
2. Franz Kafka
Kafka was of weak physical constitution and from childhood exhibited high emotional overexcitability. He was extremely sensitive and irritable. Already as a child he was humble and lacked any artificiality. His interest and emotional involvement in literature showed up very early. In the course of his maturation this interest underwent a transformation to become an attitude of sacred mystery.
From childhood Kafka showed a maladjustment to the practical side of life and in the opinion of his friend, Max Brode, “he had too little taste for possessing the things of this earth.” On this background developed his general culture, his modesty, his uncertainty and complete inability to make decisions about his own life. On the background of his emotional overexcitability and introvertive sensitivity he developed abilities for exceptional insight and discussion.
181
The slightest difficulties in daily living were to him insurmountable obstacles. He was very good at reading aloud writings that moved him or excited his enthusiasm but any interruption, whether to take him away from his reading to eat breakfast or to change dress, brought on such a strong reaction that he either trembled all over or lapsed into silence unable to move.
His overexcitability and general sensitivity were the reason that he could not bear his father’s behavior who always reprimanded him, corrected him and yet at the same time was coarse and the very negation of his injunctions.
His attitude towards his father was, in our opinion, not an expression of an Oedipus complex but of a total contrast of type, an expression of a protest against his father’s type and behavior, a protest of a man full of subtlety, endowed with a great depth of reflection and complexity against a type who was primitive, authoritarian, without any capacity for inner psychic transformation, lacking deeper emotional contents. With his mother Kafka did not have a good relationship and understanding but he did not hold any resentment against her.
Kafka was afraid to be observed by others and reacted with anxiety when people paid attention to him. One can say that the influence of his environment (his family) was sufficiently strong to develop in him this particular sensitivity. In this case his developmental potential rather than counteracting this influence yielded to it.
In his creative thinking Kafka became aware of the worthlessness of speaking. He maintained that only that counts what cannot be put into words. According to Albérès and Boisdefferre (1968) Kafka was blinded by Truth and at the same time was a genius of the absurd—a man who was searching for truths that are not only unknown but also incomprehensible in his time. Kafka’s world was composed of three realms: dreams, creativity, and everyday reality with which he felt the least in common and which often repulsed him. He felt more at home in other levels of reality. The world of his dreams became his real world. Contrary to the usually experienced fragmentation, unreality, and discontinuity of dreams Kafka’s dream world had a distinct continuity and a distinct relationship to the realities
182
of human existence. The transposition of his main current of activity to the dream world was for Kafka also a means of handling the difficulties of everyday life.
He gradually systematized the world of his dreams and it became the source of his creativity. According to Albérès and Boisdefferre (1968, p. 67) Kafka by his “dry” concern with detail created the real in the unreal. The worlds he called into being appear incredible, yet they exist.
The exclusivity of his devotion to literature increased his dislike of that which did not belong to the sphere of creative writing. To him writing was a form of prayer. By depicting the absurd which encompasses our whole reality, by his extremely penetrating grasp of the antinomies of human existence Kafka has undermined our faith in the plane of reality which we normally see. A trial without a prosecutor and without defense with only the defendant present, the metamorphosis of Gregor Sams into a cockroach during his sleep, the characterization of behavior common to insects and men, these are Kafka’s nightmares that have shaken up human complacency and ontological security with greater power than any other literary creation. By describing life reduced to the absurdity of the life of a cockroach who has a subconscious feeling of importance although his existence is without any significance, Kafka depicted the dread of small human affairs which grow within limited “awareness” to the order of ominous significance. The symbolization of the “logic of human reasoning” in the behavior of an insect (“Metamorphosis”) reflects the dread of the meaninglessness of the ordinary human relations and behavior. He was showing by this the disproportion between the accepted reality and what it actually is.
In the main character of “The Trial” and in “The Penal Colony” Kafka gives concrete examples. Of how man has hopelessly, irredeemably locked himself by his own laws and social conditions. The allegories of human reality developed by Kafka have anticipated concentration camps, the death of millions of people and the agony of their suffering.
In his dreams Kafka was a realist. These dreams were formed into a synthesis and a system of higher reality. Saying that every human being has to lock himself, he locked himself
183
in the world of his dreams. His strong insight into himself is shown by his saying: “the human being has his awareness imprisoned in the body.” According to Albérès and Boisdefferre (1968) Kafka has cast, through his suffering and insight into human existence, a prophetic shadow on the future of mankind. His realism was apocalyptic.
Kafka was an irrational creator on the highest level. His visions were fantastic and dramatic, yet at the same time they were elaborated into a system with its own logic. Kafka’s creativity was never the result of automatic dynamisms (i.e. without inner psychic transformation) but sprang from high awareness based on emotional experiences and dreams. His creativity was associated with such characteristic psychoneurotic needs as isolation, solitude, and such reactions as anxiety in meeting people.
The moving forces of his creativity were the exaltation of a priest and the patience of a craftsman. During writing “Amerika” and “Creative Metamorphoses” he was in ecstasy. Frequently he was experiencing guilt, was full of anxiety; these feelings, although disturbing, acted as a trigger of his creative ability.
The feeling of being observed and being guilty was one of the essential contents of his psychoneurosis (perhaps even schizoneurosis) and became one of the leading themes of his writing.
The dynamisms of reflection, complexity, and emotional sensitivity operated in his creative output and were related to such things as: escape from ordinary reality, protest against brutality, sharp sense for detecting dishonesty, hypocrisy and other primitive forms of behavior in his environment.
His protest against excess of material preoccupations, against the discrepancies between professed opinion and actual behavior (his father) were shown in his psychoneurotic and creative processes. Of course, we consider his psychoneurotic behavior as a positive (i.e. developmental) phenomenon. Kafka is an excellent example of a developmentally positive psychoneurotic and his creativity is clearly psychoneurotic. His excessive need of solitude and of realizing his creative goals were for him the needs of highest tension and were also his curse.
184
In his behavior he was uncertain, hesitant, especially in relation to marriage. Thoughts of death as a liberation from his difficulties were his constant companion. He had self-destructive tendencies and always had, thoughts of suicide. He felt that there was, something incorporeal about him. He lived in the world of essence and spiritual concreteness. By his continuous hesitation he repeatedly brought himself to exhaustion. At a certain moment he began to love his fear as a creative element.
Mortally ill he was extremely productive. His illness provided for him the conditions free of disturbing distractions. But there was a breach in this—from Kafka’s point of view—ideal situation. There appeared in his life a new value, a strong rival to literature, namely a great love. A woman came to share his last illness and the love for her embraced him totally.
Analyzing Kafka’s behavior and development one can say that his psychoneurosis was equally strong as his creativity and that the two meshed closely. Kafka had said about himself: “What I have achieved is the success of my solitude.” He also said that what he could give to a woman he would have to take away from literature. In the context of his development it would appear that this decision was right and is a witness to his own way to wisdom. His exclusive dedication to his literary visions gave his life a great richness of which his writings are an example evidence.
Kafka’s life is a prime example of the role of psychoneurotic dynamisms in development. His extreme sensitivity and excitability, primarily emotional and imaginational, were the basis of his nervousness, and together with his creative literary potential compelled him to escape into solitude and a world of imagination and dreams. He removed himself from contact with everyday reality. He owned nothing “in this world.” Attempts to disturb him in his preoccupation with essences lying totally beyond everyday life caused him to react drastically, as described earlier, by excitation or immobile withdrawal. These distinct psychoneurotic reactions are also evidence in his case of thirst for creative saturation and of creative nostalgia.
185
Kafka could not tolerate being observed suspecting in such behavior shallowness and aggressiveness. He did not tolerate small talk. Feeling the worthlessness of talking he isolated himself more and more from ordinary contacts and dived in his own “essence,” dreams and writing. He observed the mechanisms of ordinary human life, its “insect logic,” hence his portrayal of one-sided development as something anti-human.
He had anxieties and feeling of guilt but at the same time he made use of them, almost ecstatically, in his writing. (“The Trial,” “Metamorphosis,” “Penal Colony”). With his writings and his life he protested against verbalism, “logic,” and the hypocrisy of everyday life. His “psychoneurotic” pains, anxieties, obsessions, Kafka transformed into creative material.
3. Gérard de Nerval
Gérard de Nerval was a prominent French poet of the romantic period. His poetic abilities were displayed early in his life as well as his enhanced emotional and imaginational excitability. These traits were deepened by grave experiences of his life: early death of his mother, feelings of abandonment, emotional disappointments later in life. He grew defenseless and in need of affection to feel protected and secure.
His whole developmental potential was based on an inborn poetic talent and these two forms of overexcitability, which gave him more occasion for the tragic and sad experiences than the pleasant ones. He did not exhibit any interest or need for systematic development of his own poetic style.
The high degree of his poetic perfection grew together with his enhanced emotions and imagination, with a growing separation from reality, with an always present need for idealization and a need for love. His visions, dream experiences, daydreams, or states of separation of his “astral double” were the source of his richest experiential and creative material. He commented on his experience during his illness while under the care of his psychiatrist and friend Dr. Blanche: “It was never easier
186
for me to carry out an analysis or description than under the conditions of my illness” (Richer, 1962, p. 83).1
He was given to animism, magical thinking, faith in the total reality of a supersensory world. These are traits of positive infantilism [see Chapter 5, section 1 (6) (note l). With the passing. Of years these traits were, so to speak, perfected by him without adjusting to the requirements of everyday life.
The essential creative elements of Gérard de Nerval’s poetry were arealism, imagination and fantasy. We can, I suppose recognize here the realism of a world of fantasy with strong. Contemplative components, if such perceptions are strong, wide and systematized. De Nerval, practiced some form of meditation fairly regularly. As a result he experienced states of autosuggestion, trance, premonitions and visions. Such elaborated world of imagination in spite of being removed from ordinary reality has its own sense, its own limits, its own organization, its own laws independent to a large extent from the laws of the ordinary reality. According to Richer (1962) all of de Nerval’s visionary, symbolic, obsessive elements together-expressed his “unceasing care to endow the smallest detail of individual character with a universal significance” (p. 82).
Such a world gives an experiential satisfaction to those who dwell in it. To Kafka it was the world of his dreams, to Proust it was the world of his memories, and to Gérard de Nerval it was the visionary world of persons, events, and symbolicized premonitions.
_________________
(1) An American poet Theodore Roethke at the time when he was approaching a major breakthrough in his writing recorded this in his notebook: “Why do I wish for an illness, something I can get my teeth into?” (Seager, 1968). Roethke was hospitalized several months later on a psychiatric ward. Seager made use of the theory of positive disintegration to account for this episode and to explore its possible relation to Roethke’s major poem “The Lost Son.” Roethke’s development and creativity are an excellent example of the process of multilevel disintegration; its later, more mature, and more deeply reflective content are expressed in such poems as “The Meditations of an Old Woman,” “The Dying Man,” “North American Sequence.”
187
Inspiration came to him easily, it was rich in fantasy and emotional explosions which expressed his inability to adjust to ordinary reality. One may say that he was not highly conscious of these processes but the fact of their spontaneity does not make his creative process something automatic. Judging from the creative and magical elements of his poetry based on enhanced emotions and imagination one can suppose that he had visions of living persons, imaginary characters, and ghosts. Richer (1962) said that de Nerval’s states of greatest disequilibrium were related in time and in content with his most creative periods. At such times he produced his most outstanding works, such as “Les filles du feu,” “Les chimères,” and “Aurélia.”
His whole life Gérard de Nerval carried in his heart a mourning after his mother who died when he was very young. As a result he was always looking for an exclusive love relationship which would combine the ideal of a mother with the ideal of a lover. Often he displayed romantic exaltation which was also a cause of errors in his evaluation of his loved ones (e.g. Jenny Colon).
It seems clear that such traits as his enhanced emotional and imaginational excitability, his infantilism, his feelings of inferiority, his exaggeration of exclusive and intimate emotions, his illusions and visions, were related on the one hand to his poetry, and on the other to his psychoneurotic constellations.
Gérard de Nerval was clearly a psychoneurotic. The evidence is in his life, his creativity and his death. He had a strong feeling that fate was governing his life, and since it was forecast for him that he would die by his own hand he eventually hung himself in order to bring his fate to its final conclusion.
His interests, his states of split personality are easily discernible in his works saturated with sensualism, mysticism and mediumistic states. He was the precursor of symbolism and surrealism. Symbols taken from alchemy, Tarot and mythology play an essential role in his writing. The things he experienced like delusions or visions and hallucinations, had for him fundamental significance as a contact with higher reality. He said in a letter to Dr. Blanche: “Perhaps these strange things that
188
I experience exist only for me … whose brain has difficulty in separating the real life from that of a dream” (Richer, 1962, p. 88). De Nerval believed in the influence of stars on human life, reincarnation, and that everything in the universe has life (he was not different in this last belief from Alfred North Whitehead).
Can we speak of Gérard de Nerval’s wisdom? We see a considerable degree of naiveté, childishness, and maladjustment to practical things. Thus his practical I.Q. was low but his intuitive I.Q. was high. He was also capable to exhibit at times a high level of stoic attitude, subtlety, trust, delicateness and high moral responsibility. Often short of money he was nevertheless generous. He often helped other writers with advice and personal attention. He was sensitive and delicate in his relationships of friendship and love—he was capable of closing certain feelings within himself and at times exercising a very strong control of himself. We can, therefore, regard it as an expression of some form of wisdom, even though only partial, one-sided and impractical.
Let us try to outline the relationship between de Nerval’s psychoneurotic dynamisms, his creativity, and his development.
Like in Kafka’s case his enhanced excitability was mainly emotional and imaginational. His exclusive, ecstatic, all encompassing love for his mother were one of the strongest factors in the shaping of his development and his creativity. His enhanced excitability and the trauma of his mother’s death were the basis of his maladjustment and his creative impulses. He isolated himself from reality and dwelled in the world of fantasy, esotericism, idealization of love. His occult experiences account for his irritability, lack of reality function at a low level, but at the same time for the factors of his creativity and individual development. His faith in the supersensory world was a strong creative factor but also it was an expression of a neurotic “absence” to realities of everyday living, and lack of adjustment to it.
Gérard de Nerval combined childlike, even psychoneurotically infantile traits of sincerity, animism, magical thinking with creative inspiration soaring into a romantic and ideal world. Nevertheless he was systematic in his efforts to develop his eso-
189
teric experiences, visions and dreams by regular meditation. Like Proust he created a “reality” of visions and presentiments.
In his behavior he was queer, neurotic, sometimes bordering on psychotic symptoms. Yet the periods of his greatest disequilibrium were also the periods of his greatest and most fertile inspiration. In his writings, visions, “infantile” experiences, feelings of inferiority, exclusive and ideal bonds of love, make up the theme of essence and of his developmental path. He was conquering a “higher reality,” he created and died in the manner of a psychoneurotic, yet a manner that was autonomous and authentic even though one-sided. It was this in him and in others like him which paved the path for symbolism and surrealism. A stoic attitude towards poverty and life difficulties together with such intense creativity are to a great extent the hallmarks of a “psychoneurotic self-direction” of de Nerval’s development.
4. Jan Wladyslaw Dawid
Dawid was an eminent Polish psychologist living at the end of the 19 th and the beginning of the 20 th century. His research interests combined both the empirical and the behavioral type of investigations of intelligence, motivation for work, etc. His attitude appeared to be primarily that of an intellectual with a fairly limited emotional syntony.
Under the impact of his wife’s suicide his psychic structure, his psychological type and his methodological approach underwent a basic change. From a cool logical empiricist he became an individual sensitive and alert to the feelings and thoughts of others. He recognized in himself a reed for parapsychological experiences and began to work on inner feelings, mystical experiences, and especially contemplation and ecstasy. In this work he did not lose any of his previous clarity of mind, precision of observation and formulating conclusions, nor gave he up logical reasoning. He was then over forty. One can say that with this fresh start he transcended his psychological type and his biological life cycle.
His creative output grew out of his gravest psychical traumas which changed, accelerated and gave direction to his develop-
190
mental potential that until then appeared to be largely hidden.
Dawid himself remarked on how decisive in bringing about this change was his wife’s death. He said that his previous research by comparison had hardly any significance in giving him a sense of meaning for his life and his work. The tragic circumstances were the main cause which released his genuinely creative experiencing and thinking. In this he had only one goal: to penetrate empirically (mainly by means of meditation and ecstatic states) into the supersensory world. His whole creative potential focused on the area of psychic development which as if unveiled itself before him after the tragedy of his life. His books like “Psychology of Religion,” “Last Thoughts and Confessions,” “The Soul of Teaching” demonstrate his fundamentally new conception of reality.
Dawid himself has said many times that in his “realistic period” he was much less creative than in his later phase of life. Using Maslow’s descriptive terms one could call Dawid’s first research period to be “deficiency-motivated,” and his second research period “growth-motivated” (Maslow, 1966).
This outline of Dawid’s life and scientific career shows that his mode of thinking first underwent a disintegration, then enrichment with the transcendental dimension. It increased the depth and the scope of his thinking while preserving the empiricalness and the precision of his methods.
Dawid’s creative process was in general conscious, although some contents had an unconscious, or even superconscious character embracing mystical phenomena. Such were his high intuition, empathy and the feeling of the presence of his deceased wife near him; also the feeling that his wife spoke to him although he was aware of uttering the words himself. He became convinced that the way to mysticism broadened, deepened and elevated his awareness and was the cause of his greater understanding of others and empathy. Nevertheless, both during his experiences of higher states of consciousness and afterwards he elaborated them critically and systematically. He studied with discrimination available sources on mysticism, parapsychology, methods of self-perfection and meditation. Dawid himself began to practice meditation as an empirical approach to the study of mystical
191
phenomena. In consequence his attitude towards people became more deeply empathic.
As was mentioned before, Dawid in his “realistic period” paid little attention to the emotions. He was strongly introverted. Yet under the cover of self-control and rationalism one could perceive emotional tension, excessively sharp criticism and occasional explosiveness. This indicates that he was endowed with emotional overexcitability but subjugated it to precise and detached thinking.
In his second period his emotional attitude underwent a decisive expansion in depth and calm. It is then that he developed empathy, greater creativity and a need for mystical experiences.
As for the relation between psychoneurotic symptoms and the development of personality, Dawid regarded himself as a different and changed man, a mystic with a totally transformed personality. He was also considered as such by the people who knew him and who worked with him, however, many psychologists and teachers who had little contact with him suspected him to be psychotic.
We have here a confirmation of the relation between the development of personality and the development of psychoneurosis (nervous breakdown, depressions, anxieties, intensive search for mystical solutions) and growth of his creativity (new horizons of thinking, new conceptions, new methods of work) and a new and more affectionate attitude towards others—an un-covering of the inner psychic milieu.
We can ask now whether his work had a neurotic character since Dawid himself can be considered a psychoneurotic. In the second period of his life he actually was a psychoneurotic, which in our view means that he gave evidence of undergoing accelerated development both in his personality and in his writings. The psychoneurotic elements of his written output are evident in expressions of despair, depression, autistic thinking, occasional visions, and even telepathic conversations with his dead wife.
In contrast to his earlier field of interest which was narrow both in method and scope, in his second period he displayed
192
universal range of interests and greater complexity of his scientific attitudes. This increased range of scientific possibilities of research was exemplified by the fact that he gave attention to the significance of experiencing in development, that he discovered for himself the highest levels in meditation and ecstasy, and that his empathy has grown to a high degree.
Dawid’s process of development of his personality has led, in our opinion, to the evolution of his wisdom. This wisdom was expressed in the combination of the faculty of intelligence with empathy, and in his multidimensional and multilevel perception of reality.
5. Ludwig Wittgenstein
In the eyes of his university colleagues Wittgenstein was universally brilliant in philosophy, mathematics, architecture, and music. Yet he suffered mental disorders bordering on insanity. His biographer says that all his life Wittgenstein was on the verge of mental illness (Malcolm, 1958).
Wittgenstein was open, sincere, without any artificiality. His ideas were often misunderstood and distorted even by some of his students. He did not seek influence and actually did not appreciate the weight of his influence (Malcolm, 1958).
Throughout his whole life he was afraid of being run over in the street. Basically he was very unhappy. He neglected his appearance. He had conflicts with others because of his capriciousness and unevenness of behavior. He was sensitive to the needs and tribulations of others to whom he easily gave away money; he had no talent for practical affairs. Also he had no inclination to influence others, to assume special attitudes, or to develop a style of life.
From childhood he gave evidence of his abilities and intelligence and unpredictable behavior. He manifested severe states of anxiety and depression. He was given to inspiration when he felt he was about to catch a problem in its nascence. It was easy for him to get visibly excited by some questions raised in seminars. He hated lecturing and lacked order. It was hard for him to stick to one piece of work, he had to shift from one kind of work to another. In contrast to his restless behavior he had a great need for being alone.
193
His thinking was original and based on rich intuition. His creative process had an inspirational character. Creative ideas came to him on a wave of tension of feeling and imagination. He was the extreme opposite of a calm and recollected creator. Wittgenstein negated stereotypes in thinking and negated conventions in ordinary life.
The relationship between Wittgenstein’s development of personality and his psychoneurotic processes was very close. His best ideas were the result of periods of greatest isolation, depression, fears, and tensions related to a strong pressure of changing contents which made him move from one thing to another.
All his life Wittgenstein was very critical towards himself and was capable of correcting his behavior. In his life he was more and more paying attention to essence. These characteristics are evidence of his continuing conscious inner psychic transformation.
He was forgetful about everyday matters, he was beset by depressions, fears, sexual difficulties, which adds up to a summary picture of a serious psychoneurosis. His death remains an unresolved mystery, although there are valid indications of suicide.
We have mentioned before the high level of his intelligence, ability, sincerity, empathy, and openness. Wittgenstein presents us with a case of restless wisdom. In the opinion of many he maintained his wisdom in spite of his psychoneurosis, and in my opinion, because of his psychoneurosis.
6. Psychoneurotic Dynamisms and Personality Development
On the basis of these four examples of outstanding personalities and the clinical cases we shall try to formulate hypotheses about the relationship between the sources of development, changes of the principal dynamisms of personality and the higher psychoneurotic dynamisms.
In both the phenomena of personality development and the psychoneurotic processes we find:
1. Psychic overexcitability in its different forms is present together with nuclei of the inner psychic milieu, nuclei of spe-
194
cial talents and abilities, and the need of becoming aware of one’s own developmental process. We see this in Kafka, de Nerval, Dawid and Wittgenstein and in the clinical cases no. 2, 3, and 6.
2. The processes and symptoms of unilevel (Cases 1, 4 and 7) and multilevel (Cases no. 1, 2, 3, 5 and 6) disintegration, whether partial or more global, lead to a partial or more global secondary integration. In contrast to most clinical cases all outstanding personalities represent multilevel disintegration. Dawid and cases 3 and 6, and to some extent 2, show a distinct trend toward secondary integration.
3. Strong elements of positive maladjustment to both the inner and the outer milieus are manifested by a tendency (more pronounced in personality development) to strive for that which “ought to be” (striving for self-perfection). All clinical cases and all outstanding personalities demonstrate higher or lower degree of positive maladjustment. Cases 6, 2 and 3 and all outstanding personalities show also strong maladjustment to some traits in their own psychological make-up and their own growth process.
4. Tendencies for the development of the inner psychic milieu, are manifested by the presence of characteristic multilevel dynamisms such as astonishment with respect to oneself and the environment, disquietude with oneself or one’s relationships, dissatisfaction with oneself, feelings of inferiority with respect to one’s own possibilities and to the environment, feelings of guilt, “subject-object in oneself,” the third factor, inner transformation of stimuli, disposing and directing center at a higher level, activation of the personality ideal. The presence of these dynamisms indicates an increasingly more autonomous development of the psyche taking place through the disintegration of lower tendencies and building a higher inner psychic milieu The names given to these dynamisms reflect the deepening “division within oneself” between higher and lower dimensions of reality.
These dynamisms have been described in more detail elsewhere (Dąbrowski, Kawczak and Piechowski, 1970. Most of them are evident in Cases 6, 2 and 3, some in 1 and 5.
195
In Kafka, de Nerval, Dawid and Wittgenstein all these dynamisms are prominent.
5. Realization of tendencies for inner psychic transformation. Inner psychic transformation is initially based on the development of the above-mentioned dynamisms. Inner psychic transformation as a dynamism in its own right is the out-come of a synthesis of most of these dynamisms, of awareness of the process of transforming oneself, of the realization that some permanent changes have already taken place in the course of self-directed development on the way to achieve one’s personality ideal, and that other changes are to follow.
Inner psychic transformation is very clear in Dawid and Wittgenstein less so in Kafka and de Nerval. It is very strong in Cases 6, 3, and 2, and much less so in Case 5.
6. Creative abilities connected with hereditary endowment appear in both psychoneurotics and outstanding personalities. Their expression is a positive maladjustment to ones; if and to the environment and a search for new higher ways of understanding reality and of creating or discovering these new ways. Creative abilities are the outstanding trait of Kafka, de Nerval, Dawid and Wittgenstein, and are also present in Cases 2, 3, 6, and partly 5.
These creative tendencies are evident in the genesis and development of the inner psychic milieu, in the sensitivity to stimuli form the external milieu, and in the tendency for accelerated development. Both groups of phenomena (psychoneuroses and outstanding personality development), apart from their similar hereditary endowment, are subordinated to the process of positive disintegration as well as to accelerated development through crises. Inner conflicts often lead to emotional, philosophical and existential crises. Both represent tendencies towards internal autonomy and authentism.
Taking particular dynamisms and processes into consideration we would like to stress that, for instance, when a depression increases our feeling of inferiority in respect to ourselves, when it introduces a sense of humility, when it brings in sadness, then by this it builds autonomy, authentism and augments
196
the striving for the ideal. When an existential anxiety develops then it is an expression of both a psychoneurosis and personality development.
The higher the functions in psychoneurosis, the more one uncovers elements of personality development in the subject, the stronger are the dynamisms of inner psychic transformation operating on such pathological phenomena as obsessions, depressions, and anxieties which at higher levels lose their pathological character. This means that the positive development of psychoneurosis becomes identified with the development of personality through the participation of the creative instinct with the instinct of self-perfection.
Comparing main elements of the development of psychoneurosis and personality it is necessary to direct our attention to the problem of stages of development of both psychoneuroses and personality. From our observation, we can conclude that in lower forms of psychoneurosis, such as primitive levels of hysteria and hypochondria, strong developmental factors are lacking. But it is, we believe, also clear that even in such forms and levels of psychoneuroses, the developmental possibilities are still greater than in the so-called normal but rigid, primitively integrated structures and even more so than in the rigid psychopathic and mentally retarded structures.
We mean here that psychoneuroses on a medium or even law level of functions express certain sensitivity to external and internal stimuli, certain instability of attitude as an outcome of their sensitivity and in this way give some hope for change (i.e. a developmental change). This phenomenon is absent in psychopaths or in lower level retardates, or on the borderline of normality and psychopathy.
7. The Role of Creative Dynamisms in Psychoneuroses and Types of Development
(1) Creative dynamisms in unilevel and multilevel disintegration.
On the basis of observation, clinical experiments and some systematic clinical investigations we cannot be sure that some of our opinions in this area have been sufficiently verified. We
197
can generally say, however, that psychoneuroses which are associated with processes of multilevel disintegration are expressive of a greater creative drive than are those psychoneuroses which correspond to symptoms of unilevel disintegration. Generally it may safely be taken that the lower is the level of function represented by a given psychoneurosis, the fewer creative elements are involved.
All developmental dynamisms are creative in a broader sense. The higher the level of development the closer is the link between creativity and developmental dynamisms. More specifically, creative dynamisms are represented by different abilities and talents, search for “otherness,” for non-stereotype components of reality, inclinations to be astonished, anxious about actual reality, and in consequence finding oneself maladapted. Other examples of creative dynamisms are enthusiasm, empathy combined with strong emotions, rich conceptions, plans and programs with a discernible multilevel character, profound identification with people, with nature, and with one’s “higher” self.
Lack of creative tendencies goes together with lack of inner conflicts, lack of positive maladjustment. One finds more of stereotypy, rigidity, lack of attempts toward developmental solution, all of which is a manifestation of lack of creative coping with life, of a “psychic dwarfism.” And so, the least creative tendencies are found in hypochondria, neurasthenia, sexual and lower forms of hysteric neuroses. Greater creative tendencies are exhibited in psychoneurosis of a higher level such as obsessive, anxiety, infantile, depressive or psychasthenic types.
This is caused by the fact that in the higher psychoneuroses we have a preoccupation with general or existential problems frequently of alterocentric character full of inner conflicts and attempts at their resolution; there is also a preoccupation with fundamental moral, philosophical, and transcendental questions. In contrast, the lower psychoneuroses such as hypochondria, hysterical conversion, sexual neurosis, and the like, do not show this type of preoccupation, awareness, and striving for resolution. The higher psychoneuroses present us with a picture of obsessions of heroism, self-sacrifice and responsibility, fears
198
for the future of mankind, or excessive universal sensitivity of infantile type. Again this is not observed in the lower psychoneuroses because perceptions are narrow, experiences are limited, and the general orientation is egocentric. In the higher psychoneuroses we have “seeing” of new things, answers to the meaning of life, a search for the “new and other,” separation into levels, tensions accompanying the search while in the lower ones we have stereotype tendencies and perceptions.
It may be taken as a regularity, that, the more pronounced is the process of multilevel disintegration, that is to say a process allowing for personal awareness of distinct levels of life and discrimination of quality, the more marked is the increase in potential for creativity, and vice versa. In unilevel disintegration the tensions are “restricted,” stereotype, without channels open “upward,” without the possibility of creative solutions, and so they tend to turn into a vicious circle, to tensions of pathological character, to uncreative collisions, which like moths break flat on the hard surface of the glass screen that bars direct access to light. In unilevel disintegration the creative talent is, therefore, more limited and to a great extent psychopathological. To name some representatives: George Sand, Stanislaw Przybyszewski, Hans Heinz Evers, and to some extent Baudelaire. They had unilevel sensitivity, weak or absent hierarchization, lack of noticeable inner psychic transformation.
(2) Types of psychoneuroses and types of creative abilities.
With regard to particular types we can say, that, for example, in the case of hysterical psychoneurosis, we often find associated dramatic talents as well as ability for pantomime and ballet (see Chapter 11). This is often connected with ambivalence of attitudes, with capacity for strong syntonic projection, for neuropathic acting, with a need for some exhibitionism, etc. People with hysterical tendencies are also often highly sensitive to sensual stimuli such as colors.
Psychoneurotic anxieties are often connected with a fair ability for observation, with psychological insight, with authentic attitudes, with the inner experience of truth and the pain of existence.
199
Among some philosophers, especially among outstanding existentialists, we encounter a history of anxieties, and also anxieties experienced often at the time of their creative writing. There is a strong concurrence of the experiences of courage, heroism, humility, fear of the unknown and the decision that one must enter the unknown, as in the case of Buddha or Kierkegaard, who spoke of fear and trembling and the courage necessary to search for the absolute, portrayed in Durer’s “Knight.” This is the relationship of the highest heroism and anxiety. We refer here especially to the “fear and trembling” of Kierkegaard, which was characteristic of his personality development and is also characteristic of the first stage of multilevel disintegration (i.e. spontaneous multilevel disintegration, or level III). Among the psychologists and psychiatrists of analytic, introverted character who are capable of self-analysis we frequently find anxious and obsessive types.
In connection with psychoneurotic depression we often deal with people who have self-critical, analytic capacities aiming at objective definitions, who are commonly given to attitudes of self-awareness and objective introspection. The process of overcoming these neuroses is characterized by an increased tendency and facility for syntony and empathy as a result of the progressive realization of a growing need for identification with others, as expressed often in literature. The knowledge resulting from one’s own suffering, from deep experience of depressions but also from overcoming them, is as a rule combined with a deeper understanding and feeling for others, with identification, and compassion. On occasion it may be expressed by outbursts of empathy in a desire to give oneself totally, as did Dr. Korczak when he went into the gas chamber with his pupils, or Father Kolbe who in Auschwitz stepped into the row of prisoners selected for death by number to replace a man and save him for his family (this man did survive the concentration camp). For Saint-Exupéry, for instance, a sense of duty was based on social sensitivity and love, and responsibility for him, to be worth anything, had to be an expression of complete self-sacrifice without expectation of a reward (Kierkegaard’s notion of “duty”).
The psychasthenic type is often characterized by originality
200
in various areas of creativity such as poetry, philosophy, literature, painting, etc. Some stimuli of a generally narrow environment to which the psychasthenic does not easily adapt may provide nuclei for the transformation of the unsatisfying reality into colorful, creative and original forms. The reality function among psychasthenics, being weak especially at a low level, is compensated for in areas of imagination and mental conceptions. In many areas of activity, psychasthenics exhibit sensitivity, insight, and originality. For this reason the success of therapy with psychasthenics often depends on the promotion of their different forms of creative abilities. They need to be encouraged to write, to paint, to express themselves. Such excess of sensitivity, originality and penetration was characteristic of Kafka in his actual practicality of some of his impractical conceptions, such as anonymous dread in social life, the hopelessness of some conditions of human existence similar to the grotesqueness and insignificance of insects. The same applies to Unamuno who gave a very penetrating analysis of the existential significance of suffering.
Psychoneurotic infantilism is characterized by childish vulnerability, maladjustment, naiveté, arealism, openness, excessive sincerity. In consequence there is great susceptibility to being hurt, general fragility, as in the case of Gérard de Nerval. The highest form of compensation is here a life in the world of imagination, fantasy, sometimes daydreaming. We observe positive regression as a need for rest in the world of carefree and sunny childhood far removed from everyday reality.
Among those subject to such infantilism we often find poetic, dramatic and artistic talents, with magic and animistic thinking, plasticity, spontaneity, informality, and expressiveness. Also in psychoneurotic infantilism we often encounter the kind of creativity which expresses the need for very strong and immutable emotional relationships, the need for dependence on other people, the need for security. This goes together with feelings of inferiority. The best example is Saint-Exupéry “The Little Prince.” We also often observe in this type of psychoneurosis the need for fantasy, for mythology, and for positive regression.
201
CHAPTER XI
SUPERIOR ABILITIES AND PSYCHONEUROSES
IN CHILDREN AND YOUNG PEOPLE
1. Methods and Subjects
The problem of superior abilities in science. Art, or any other creative endeavor, has been the subject of interest to many specialists. Particularly valuable, from the point of view of social usefulness and education, is the knowledge of the mental and physical development of gifted children and young people. In the United States of America as well as in Great Britain and the Soviet Union, a great deal of research is done in this direction. The work under current discussion was started in Poland at the Institute of Mental Hygiene and the Children’s Psychiatry Institute of the Polish Academy of Sciences in Warsaw. We were helped greatly by the Polish Society for Mental Hygiene.
We selected, from a very great number of problems, several of significant practical importance. These were problems related to superior abilities and psychoneuroses. We have not found in the literature any major attempt to discover and correlate these two sets of characteristics as we studied them in children and young people.
Of course, one should keep in mind that both our investigations and conclusions, represent at the present, no more than the initial phase of further, widely planned studies of superior abilities and that in our conclusions, we only endeavor to indicate directions, the “tender” point of the problem. These conclusions, then, should not be considered as fully elaborated permanent schemes and generalizations. On the contrary, it is our wish that the themes touched upon should encourage other
202
institutions to cooperate with us in our study of superior abilities, and also to examine critically some of the correlates indicated here.
In the following are given the results of experimental investigations of a group of gifted children and young people, aged 8 to 23. The subjects were 80 children, of whom 30 were generally intellectually gifted (from elementary schools), and 50 were children and young people from art schools (theatre, ballet, and art). One control group consisted of 30 mentally retarded children; among them 10 were examined at the same time as the gifted children; a further 20 diagnoses were taken from the card register of the author. Every child was examined by means of the best developed psychological methods and was subjected to detailed neurological and psychiatric examination. Every child was also subjected to a medical inquiry extending back to the parental period and including his hereditary makeup. The following tests were used: Wechsler-Bellevue, Rorschach, Thematic Apperception Test, special questionnaire designed to identify the presence or absence of psychoneurotic traits, detailed social interview and case study.
The neurological examination comprised methods of assessing the functioning of the autonomic nervous system (with particular attention to sympathicotonia and vagotonia), detailed examination of cutaneous and muscular reflexes, oculocardiac reflex, waxy flexibility. Special attention was given to the relation of excitation and inhibition, i.e. whether one was more dominant than the other.
A few explanatory remarks will help here.
The predominance of excitation can be observed from an excess of movements, excess of talking, quick reactions, highly dynamic responses, certain facility in making decisions, a general attitude of approach (klisis) rather than avoidance. The predominance of inhibition is observed when the above picture is reversed.
The balance between excitation and inhibition—usually variable—can be observed in the fluctuation between states of excitation and states of inhibition, and at a high level in control of excessive excitation and in excessive inhibition. At the high level this takes the form of an attitude of “being aware”
203
of both these states, and is also expressed by the presence of some inner psychic transformation and the dynamism “subject-object in oneself.” In Rorschach’s terminology it would correspond to “contact introversion.”
In the psychiatric examination attention was directed first to exclude pathological processes such as disorientation in space, in time, and in respect to the identity of the examined himself, such as hallucinations, delusions, split of personality, etc. Only individuals who did not have any of these disorders were included is the remainder of the examination. Special attention was then given to psychoneurotic syndromes, and to the correlations between special or general abilities and identifiable psychoneurotic syndromes (e.g. systematized creativity on a high level in combination with a low level of the reality function) in order to establish whether the correlation was strong or weak. The examinations were carried out in the autumn of 1962 in Warsaw schools by a dozen or so psychiatrists and psychologists.
2. Definition of Some Concepts
Since we shall dwell here on the correlation between superior abilities and psychoneuroses, we will briefly recall what we mean by these concepts.
The term superior abilities denotes abilities (in any field) which permit an individual to achieve results considerably surpassing the average accepted as standard for individuals of the same age and the same level of education. In our examinations we came into contact with two kinds of abilities: general and special. Superior general abilities were noted in children from elementary schools who were able to attain higher than average results in learning general subjects (though in practice they did not always attain these results). The I.Q. of this group ranged from 120 to 146. The general abilities were divided into humanistic, mathematical, and scientific. Children attending art schools possessed superior special abilities. Manifestations of these abilities were evident in different areas like drama, dance, art, and music. All the children examined who possessed special abilities had an I.Q. between 110 and 155.
The main factors of personality development are multilevel
204
dynamisms and conflicts, a more or less high degree of insight into oneself, an ability to control and reshape one’s psychical structure, and creative and perfective dynamisms. These factors taken together constitute the inner psychic milieu. The inner psychic milieu has a better chance of developing the more the individual is characterized by so-called psychic richness, which includes a plurality of interests and abilities, an intense emotional life, and finally the potential for accelerated development.
Because we are discussing here the relationships between creative structures, functions, dynamisms, and particular psychoneurotic constellations we employ here the traditional nosological units of psychasthenia, neurasthenia, anxiety neurosis, neurotic depression, hypochondria, hysteria, and sexual and somatic neurosis.
We assume that within the scope of the same kind of neurosis every syndrome may have, in general, three different degrees of intensity.
The most serious degree is one of a distinct neurotic or psychoneurotic disorder (e.g. distinct disorders of the reality function, strong aggressive or suicidal tendencies, difficulties in studying, or distinct psychosomatic disorders).
The medium degree presents an “average” level of transient disturbances, which, nevertheless, recur often.
The weakest degree is one, for example, of fleeting symptoms of nervousness, neurotic, or psychoneurotic disorders, often not noticeable externally, and, which do not leave permanent traces in the psyche (e.g. symptoms of increased psychic excitability, passing psychomotor disturbances, slight play-acting, impulsive actions, lability of mood’s).
3. General Characteristics of the Children Examined and Individual Examples
Every one of the children investigated showed considerable psychomotor, sensual, affectional, imaginational, and intellectual mental overexcitability. Moreover, it turned out that these children also showed sets of nervousness, neuroses and psychoneuroses of various kinds and degrees of intensity, from light functional symptoms, or anxiety symptoms, to distinctly and highly intensive psychasthenic or hysterical.
205
The identification of such combined sets allowed very rich descriptive diagnosis characteristic for each child. For example enhanced excitability without concomitant inhibition is an expression of lack of control, but excitability and sensitivity with inhibition demonstrates not only sensitivity of behavior but also a degree of control. These sets (e.g. psychasthenic-hysterical, anxiety-depressive, infantile-hysterical) were multilevel, combining, for instance, hysterical traits of lower and higher level, or psychasthenic and neurasthenic reactions (cf. Chapter 7, Sections 2 and 3). These are sets combining together different psychoneurotic processes. Other sets were related in a time sequence, as for instance when a strong overexcitability had a general character (dispersion of symptoms) and was periodically followed by localization of symptoms as in organ neurosis. One of the female patients expressed it thus: “I am ‘wandering' from one category of symptoms to another, from such that are spread all over and ill-defined to those which are well-defined and take up an identifiable spot.”
With the children and young people investigated, certain definite psychoneurotic sets predominated, namely medium degree anxiety neurosis (about 30 percent), medium degree hysterical sets (25 percent) and light intensity neurasthenic sets (25 percent). The examination also revealed a considerable amount of psychasthenia and somatic neurosis to the extent of about 10 percent each. Of course, each of these sets greatly differs in particular cases, depending on the child’s age, kind of interests and abilities, type of school, environmental conditions, etc. In the period of changes in respect to oneself and to the environment, its customs and moral standards, hysteroidal symptoms will be different in a 10-year-old (fluctuation of mood, capriciousness, suggestibility) from adolescence and puberty (symptoms of conversion, emotional-psychomotor crises, ambiequal tendencies for adoration and antipathy).
Creative abilities enable one to a large extent to gain a higher level of the psychoneurotic process, which in consequence makes prophylaxis much easier. The school or the family may significantly help to reduce the symptoms, and with an understanding of the child’s difficulties—even prevent a nervous breakdown or suicide. We also observed multi-formed connections between
206
these sorts. The pictures of the neurotic and psychoneurotic sets were very rich and differentiated. Below we give an example of a syndrome of anxiety neurosis with neurasthenic and hypochondriacal components:
Neurological examination:
(1) Case 15
A boy, 8 years old, in third grade of an elementary school, good educational environment. Doing very well in all school subjects; I.Q. 136 Wechsler test. Creative ability in drawing. Theoretical and humanistic interests.
Pupils quite dilated, strongly trembling eyelids and trembling of hands. Increased abdominal reflexes. Increased psychomotor excitability of a constricted type. Tic-like movements. Increased muscular tension. Dreams about fears and persecutions. Distinctly waxy flexibility (flexibilitas cerea). This neurological examination reveals great psychic tension and difficulties is finding release from it (tic-like tendencies). Inclination for an organ neurosis is likely (enhanced abdominal reflexes). The trembling of hands and eyelids, dilated pupils, general anxiety and excitation combined with inhibition seem to indicate tensions of expectation and searching.
The boy appeared to have a good contact with his environment. A subtly administered system of praise would be recommended here to strengthen his self-concept and his acceptance by his peer group. Under some conditions he avoided people and was timid in new situations He looked for help from adults. He lacked self-dependence. He was inhibited, helpless, and not sure of himself. He had strong fear of suffering injustice, and feared the possibility of losing his mother, feared the schoolteacher’s castigation, feared sickness, hospitalization and physical effort. He was afraid to be late for school and left home much too early. He was afraid to sleep alone, or to remain alone in a room. Periodically he showed opposition and out-bursts of aggression which left him very tired. He was impatient, easily got angry and cried. In school work he was uncertain of himself, forgetful, trembled, and gesticulated. He had great difficulty in concentrating. Easily discouraged, he had an in-
207
clination to pessimism and believed he would never succeed in doing things. Sadness and the feeling of inferiority were dominant. Yet he was diligent and systematic in his work to an exaggerated extent. He avoided sad books and emotional films. He was also affectionate.
It is fairly obvious that it cost this boy a lot to maintain a positive attitude toward his school environment and to try to meet its requirements. He had difficulties in opening up, in developing contacts with others which intensified his fear for those closest to him (mother) to the point of obsession, and also augmented other fears (he was afraid of being put in a hospital). His tension, sometimes impossible to overcome, made him gesticulate, tremble, occasionally scream. The distinctly positive characteristics of this boy are: his close relationship with his mother, fear of injustice, excessive feeling of responsibility, systematic approach to his tasks as compensation for his anxieties and lack of concentration.
His developmental potential can be seen in the combination, of his fairly high excitability with inhibition, in the combination of his sensitivity, impatience and anger with states of anxiety, and above all his sensitivity to unjust treatment, his strong, relationship with mother, a feeling of inferiority in respect to himself, and his feeling of responsibility and systematic approach to his schoolwork.
(2) Case 16
A girl, 20 years old, with favourable home background. I.Q. 116. Superior ability in all general subjects, plus dancing and. Acting.
From early childhood she had fits of capriciousness, bad temper, and suicidal threats; she blackmailed those closest to her.
At the time of the examination she suffered from headaches, giddiness and heart pains without apparent reason. In addition she had disorders in breathing, difficulties in falling asleep; nausea when caught by an emotion; allergy to the odors of ether and benzene. When in anger she easily fainted. Her body, extremities were cool; her hands and feet moist. Psychomotor
208
reactions and thinking processes were accelerated. She could not concentrate.
She was nervous, touchy, chatty, noisy, complaining. She smoked cigarettes, had an uneven appetite. She was claustrophobic and afraid of loneliness. The tempo and the quality of her work depended on her mood. She bad outbursts of joy and periods of shyness. Her interests were one-sided and she spent much of her time seeking new thrills. She showed mannerism of behavior. When in states of nervous tension she was capable of striking others physically.
These two cases show rather well the different ways psychic tensions can be transposed to somatic processes. This psychic somatization indicates a high degree of tension, a great general sensitivity, still weak inner psychic transformation, and great susceptibility of the organs and their systems to different constellations of psychic tensions. It needs to be pointed out that here these constellations do not fulfill a role of inner transformation, that in fact this possibility does not yet arise. The girl described as Case 16 transposed her emotional experience onto the functions of the cardiovascular system, the respiratory system (irregularities of breathing, cough), nausea and allergy, difficulties in falling asleep. Her tensions besides reaching a psychosomatic expression find release also in psychomotor and affective reactions (beating others, moodiness). Since her sensitivity has a multilevel character and because she is suggestible she appears suitable for appropriate psychotherapeutic interaction.
We can see that both cases require systematic and individual help in the sense of evaluation of their creative potential, their developmental richness and their multisidedness. It is also clear what means must be used to activate more strongly yet more orderly the forces of their developmental potential. In respect to the boy (Case 15) one would have to show him convincingly that his potentiality for development is great, and that his fears are ill founded. One of the methods would be to teach him a more humorous attitude, which with his intelligence and universality of development would not be bard. One would also have to show him convincingly the worth of his own work, which would
209
reduce his pessimistic attitude toward himself. At the same time his teachers would have to be able to see his strong sides so that they could support in him a better self-image.
In the case of the girl (Case 16) one would have to direct her interest to less rough sports like skiing, swimming in order to attenuate her aggressive tensions; to awaken in her an interest for nature and the external world. One would also have to attempt to convince her by way of example that if she tried to attain some measure of internal quietude through meditation and relaxation then her somatic disturbances would also diminish. But it would be important to convince her of her considerable abilities, and that they would flourish with more systematic and responsible effort, which needed to replace her mannerisms.
In both cases a universal diagnosis of concrete symptoms with the active participation of the subjects and a representation of the positive connections between their symptoms and their creative abilities is of fundamental significance. The psychic tension is of different kind and of different level in both cases. In the first we have excessive inhibition, anxiety, psychic contraction into oneself, excessive orderliness, while in the second, we have weak inhibition, excessive extraversion, periods of excessive need for contact, mannerism. In both cases there are strong tensions, and there is a possibility that the girl could convert her psychosomatization to a more thorough introversion. Both need to be convinced experientially about the coupling of their symptoms with their positive and creative attributes.
Each individual has his own special kind of developmental potential. This developmental potential is individually and concretely coupled with a form (or forms) and level of excitability or psychoneurosis, or both, in a set which is for the most part positive but not without its characteristic developmental dangers.
As one may see from the above examples the psychoneurotic symptoms often manifest great tension which cause frequent conflicts with the environment. They often lead to a dissipation of the positive developmental qualities, together with an upset-
210
ting of the possibility of the development of exceptional abilities. These individual nuclei of child’s personality endow him not only with his own psychological type, be it introvertive or extravertive, schizothymic or cycloid, enhanced excitability of imagination, affect, etc., but also with differentiated nuclei of the inner psychic milieu, various nuclei of interests and abilities, and consequently with different scope and level of awareness and self-awareness.
4. The Inner Psychic Milieu and the Kinds and Levels of Psychoneuroses in Young
People with Superior Abilities One may ask what is the origin of the increased tendency among gifted children, who have good conditions of life and learning, to become subject to psychoneurotic states. The origin lies probably in the constitutional hyper-sensitivity toward the whole of the individual’s experiences. An individual who has a differentiated and multilevel developmental potential not only can achieve outstanding results in learning and in work, but at the same time is equipped with an increased number of points of sensitivity to all experiences; this may accelerate “anomalous” reactions which reveal themselves in psychoneurotic behavior (Dąbrowski, 1958; Dąbrowski, 1959).
The reason why children and young people are afflicted with some and not other psychoneurotic sets constitute another problem. Most probably the cause lies in the individual personality of the child, which is specifically shaped by the multifarious influences of his particular environment. An introverted or schizothymic child who has enhanced emotional excitability may be easily susceptible to anxieties and depressions. If he also has nuclei of the inner psychic milieu, its development may be fairly universal. The extravertive type with some less pronounced elements of introversion may manifest strong emotional and sensual tensions, easy outbursts, and may have considerable difficulties in his sexual life; he may show certain hysteroidal traits, even conversion. An individual with enhanced excitability of imagination, some infantile traits, and nuclei of the inner psychic milieu, may exhibit artistic and poetic abilities and at the same time some characteristics of psychoneurotic infantilism.
211
In an attempt to show the causes of the tendency towards a given kind and level of psychoneurosis we will use the term inner psychic milieu.
The inner psychic milieu, which arises with the development of the individual, differs greatly among particular persons. The inner psychic milieu is either a multilevel or a unilevel structure. The multilevel structure emerges from the unilevel as a consequence of a conflict of value. A conflict of value is a conflict of two levels of behavior when one (the higher) is experienced as more desirable (what “ought to be”) and the other (the lower) is less desirable (“what is”). A conflict of value is a multilevel conflict and it is the first sign of an emerging conscious direction in development. With some, it is in its initial phase in which the individual has but the disposition to build the personality at a higher level. Often, however, even with older youths, we do not observe any attempt at an education-of-oneself or at a self-direction of their own qualities and abilities with a view to attaining higher individual or social values.
Among the children and young people we examined, about half did not possess distinct rudiments of an inner psychic milieu.
The presence of the nuclei of the inner psychic milieu in children and youth was tested by means of projective tests, biographical data, interviews and observations. If, for instance, there were some disturbances of the autonomic nervous system in the form of light symptoms of somatic neurosis, which the child or youth was aware of, observed, and to some extent was able to control, that was taken as an indication of some rudiments of the inner psychic milieu, although of a fairly low level. If the degree of control was higher, and the symptoms of nervousness or psychoneurosis took hierarchical forms, such as to involve some dynamisms of multilevel disintegration like astonishment with oneself, sadness or distress over one’s behavior, feeling of guilt, syntony, periodical dislike of oneself then we are dealing with fairly distinct components of the inner psychic milieu.
We can see these developmental components in Case 15; other examples are given in Chapter 1, Section 6 (1) b.
212
Whenever we observe signs of disequilibrium in the autonomic nervous systems, emotional instability, but no distinct ambivalences and, ambitendencies, and total absence of more defined dynamisms of the inner psychic milieu than such individuals were designated IPS- (no inner psychic milieu or very weak rudiments), while those with more distinct indicators of the dynamisms of the inner psychic milieu were designated IPS+.
The distribution of psychoneurotic syndromes between these two groups was as follows:
IPS+: in the drama and fine arts school psychasthenia and psychoneurotic anxiety were the most common. Hysteria was the least common. In the ballet school and in general high school somatopsychic symptoms and psychoneurotic anxiety were predominant.
IPS-: in all schools hysteria was most common, neurasthenia less common (mainly in students of drama), while the least common were psychoneurotic obsessions, infantilism and hypochondria.
We are fully aware of the limitations of the studies in respect to the size of the group of subjects and also not always distinct diagnostic picture. We can, therefore, make only very general comparisons between the two groups. The IPS+ group showed higher level of psychoneurotic processes such as psychasthenia and psychoneurotic anxiety, while the IPS- group represented predominantly lower levels of psychoneurotic processes such as hysteria and neurasthenia.
It is interesting to note that psychosomatic and somatopsychic disorders in the IPS+ group were observed mainly in the students of ballet. One can speculate, that since the primary mode of the art of dance is external appearance, body build and complexion, then there may exist a close relation between this and the interests of dancers and their environment in paying attention to the external features of reality. One could thus speculate further that the relative absence of somatic and hysterical symptoms in the students of drama and the fine arts is occasioned by the fact that these domains of art deal with larger and deeper contents and creative forms, and do not depend for their expression on artificial means of dramatization calculated for external appeal.
213
Summing up these results we may state that, with all those examined, independent of the type of school and with the presence of a rich and developing inner psychic milieu, the anxiety and psychasthenic sets increase, but when such a milieu is lacking, hysterical, neurasthenic and somatic symptoms are predominant. This means that when we find multilevel developmental factors then we also find psychoneuroses: the control of development and its disturbance occurs primarily on the psychic level. When multilevel factors are absent then the mental control and development, if any, is subject primarily to somatic control. Experienced tensions and unilevel conflicts are transposed to different areas of the body.
There appears to be a positive correlation between the lower sets in the hierarchy of psychoneurotic symptoms (e.g. hysteria) and the weak degree of insight into oneself. Likewise, there appears to be a positive correlation between a high level of psychoneurotic symptoms and a deeper insight into oneself. Which phenomenon is primary here? Enhanced excitability and psychoneurotic processes and dynamisms create a basis for a broader, deeper, more complex pattern of response to the external and to the internal reality. But on the other hand the developmental potential which is the basis of achieving this insight and the high level of the inner psychic milieu, in turn, acts further upon the psychoneurotic processes, makes them more complex, richer, raises their level, and brings about the unfolding of processes preventing negative disorders.
Further analysis showed that not only the kind but also the level of a given concrete neurosis is conditioned both by the presence of a more developed inner psychic milieu, and also by the level of this milieu. Numerous examples indicate that the localization of the same neurosis or psychoneurosis is shifted to a higher level, if at the same time the inner psychic milieu arises and develops into a multilevel structure. As we pointed out repeatedly the existential types of psychoneurosis, i.e. the higher levels of psychoneurotic processes such as anxiety, depression, infantilism, psychasthenia appear only in individuals who develop a multilevel inner psychic milieu.
In longitudinal observations many cases were recorded where a psychoneurosis of a neurasthenic or even hypochondriacal type
214
changed into medium or even higher levels of psychasthenia or a hysterical conversion changed into a higher level of a hysteroidal set with a high level of hierarchization of feelings, empathy, dramatization and contemplation. An example is given below.
A young married woman was suffering from hysteria with periodical states of stiffening of her body, even paresis, which appeared always when there were difficulties in her marriage because of psychological incompatibility, difference in interests and emotional attitudes. After several years of marriage when the couple learned to understand each other more deeply and when their mutual attraction increased as well, the young woman continued to manifest very high emotional sensitivity; empathy toward her husband and to many other close persons, At the same time she developed telepathic abilities, and premonitions of events to come with repeatedly tested reliability. In the first period of her marriage these reactions were fairly insignificant while the conversion reaction was strong, but in the later period it was the other way around. Her behavior showed the development of fairly advanced dynamisms of the inner psychic milieu such as empathy, telepathy, precognition, need of self-control and self-development. Simultaneously with this she developed to considerable degree her musical abilities and involvement in social work.
The problem raised in these pages requires further elaboration, which would involve a more exact study of inter- and intraneurotic levels of functions with a large group of subjects. At this point we would like to add several detailed conclusions concerning the kind and, seriousness of psychoneurotic sets.
When the organizing structure of personality is lacking such as the disposing and directing center on a higher level, then the intensity of psychoneurotic processes is distinctly increased, allowing the functional disorders to appear at lower levels.
Frequently in the cases of psychoneurotic anxiety of low intensity, weak “structure” of the psychoneurotics, we also find a weak structure of the inner psychic milieu (meaning the absence of the higher multilevel dynamisms). In logitudi-
215
nal observation, then, we often find that the structure of the inner psychic milieu becomes more distinct and more extensive (appearance of the activity of higher multilevel dynamisms), while the psychoneurotic process gains too in structure and intensity together with an intensification of creative power and originality of experienced contents. Very often prophylactic elements also gain in importance.
Hysteria, with very intensive symptoms and at a lower level of disordered functions, occurs most frequently when the inner psychic milieu is lacking, and vanishes almost completely when the inner milieu is developing.
In the course of development the basic form of overexcitability becomes more complex by intrusions from other forms of overexcitability. Thus in spontaneous multilevel disintegration a basic form of psychomotor or sensual overexcitability becomes enriched by appearance of components of enhanced overexcitability of affect, imagination or intellect. Likewise in the course of development a given psychoneurosis loses its “pure” character and becomes more complex by admixture of other psychoneuroses, as for instance hysteria becomes enriched by psychoneurotic infantilism, or neurasthenia by psychasthenic reactions. The stronger the hysterical sets, the weaker the symptoms of other psychoneurotic sets. The inverse is also true. Hysteria occurs to a great extent irrespective of one’s age.
With older youths the incidence of neurasthenia increases when the inner psychic milieu is lacking. Neurasthenia represents a one-sided, egocentric—even narcissistic structure. This results, from lack of multilevel, hierarchical development, in other words, from lack of development (or insufficient development) of the higher forms of the inner psychic milieu.
Psychasthenia tends to be associated with more serious neurotic states of the following types: obsessions, neurasthenia, and anxiety neurosis. In the cases of psychoneurotic anxiety at a lower level, where it is usually combined with somatization, we observe a need to find support in someone, to be in contact with others, which appears as “sociability.” When psychoneurotic anxiety attains a higher level as a function of the developing inner psychic milieu then there is also a greater tendency
216
to solve psychoneurotic problems authentically by means of autopsychotherapy.
Our rather limited study suggests that the lack of development of the inner psychic milieu (and, therefore, a greater tendency towards lower psychoneurotic processes of the hysteric, hypochondriacal, and neurasthenic type) is related to certain traits of the thinking process, such as predominance of practical intelligence, weak abstract and symbolic thinking, weak conceptual analysis, intellectual rigidity, stereotyped or disorganized thinking, agglutinative character of thinking, and an inability to concentrate. Individuals with these traits are often lost in thought, absent-minded, but they never seem to know what they are thinking about.
The arising inner psychic milieu (and, therefore, a greater tendency towards psychasthenia and psychoneurotic anxiety, i.e. higher psychoneurotic processes) is related to certain traits of the thinking process such as originality, showiness, tendency towards fantasy, magical thinking, intellectual richness and plasticity, an ability for abstract and at the same time intuitive thinking (logical yet synthetic thought), reduction of stereotype and chaotic thinking, good vocabulary and general knowledge, good symbolic reasoning, ability for concentration but not always sustained (discontinuous concentration).
Among older youths who have one-sided interests concerning only their areas of study (e.g. interests in ballet or in the fine arts) neurasthenic processes dominate. The other young people develop interests and abilities in various forms of social and personal life by further education of themselves, by studying the problems of art, by extracurricular art work, by collecting museum pieces, by ballet and singing, by learning to know nature, or by sports and traveling, in short, by more thinking, more interest, more involvement, and a wider range of creative energy and curiosity.
The development of interests, abilities and in fact the whole inner richness of the children and youths examined was accompanied by creative abilities. These abilities were very numerous and differentiated, depending partially on the age, kind of school, etc. They were revealed in special creative abilities, such as in spontaneous literary outputs (poetry, drama), in
217
individual and original interpretation of their dance, in an original painting or drawing, in composing songs, in sculpture, in pantomime, and so on. These children and youths demonstrated their developmental potential early in life.
Among older youths the majority of creative abilities was displayed by individuals with a very advanced development (i.e. multilevel disintegration) of their internal psychic milieu. We have assessed in these individuals their enhanced emotional overexcitability and initial activity of such dynamisms like subject-object in oneself, the third factor, forms of periodical self-control. At the same time we have found the following characteristics in their somewhat unexpected constellations: excessive sensitivity and subtlety, withdrawal from too easily made unselective social contract, richness of the associative apparatus, strong need for evaluation, strong artistic imagination and tendency for fabulation, difficulties. In concentrating, tendency to be easily tired, and typical psychosomatic reactions such as ease of becoming motionless while retaining awareness, temporary disorders of inner feeling (coenesthesia), sensation of possible split of the “physical” and the “psychical” self, or “picking up” disagreeable traits of other persons by touch (through handshake, for instance).
5. Conclusion:
In order to sum up we wish to stress once more that:
1. All gifted children and young people display symptoms of increased psychic excitability, or psychoneurotic symptoms of greater or lesser intensity.
2. In general, the various interests and capacities of children and young people coincide with complicated forms of psychoneurosis (i.e. with higher psychoneuroses such as psychasthenia, anxiety neurosis, or obsessive neurosis, or with a higher level of a given kind of neurosis).
3. The greater complexity of psychoneurosis as a result of the development of the inner psychic milieu contributes elements of originality and creativity. These elements are related to multilevelness of the experiential structure, multilevel conflicts, and growing self-awareness.
218
4. The development of personality among gifted children and young people usually passes through the process of positive disintegration (strictly related to the complexity of the psychoneurosis), and it leads to self-control, education-of-oneself, and autopsychotherapy, in other words, to a conscious inner psychic transformation.
5. The lower the level of global development of abilities and intelligence, the more primitive are the forms of psychoneurosis observed. They are absent in more serious cases of mental deficiency.
At this point I would like to turn our attention to my own reservations with respect to the material presented. One of the weaknesses of this study of gifted children and young people is the lack of longitudinal studies and an insufficient number of control groups. This deficiency is partly compensated by the group of retarded children (Chapter 9, Section 6) and by the author’s experiences gained from the study of children of an average mental level. We have found that nervousness and psychoneuroses are phenomena normal in the course of development. We should therefore look upon the majority of forms of nervousness and psychoneurosis as indicators of developmentally “normal” phenomena.
We think that we shall have reached our goal if this work will focus attention on the positive relation between the development of superior abilities and talents and the development of psychoneuroses in the direction of their higher forms. The practical conclusions may be drawn by psychiatrists, psychologists, educators and all those dealing with the problem of outstanding abilities. Such an approach, if accepted by the centers deciding about our education and culture could bring it about that nervous and psychoneurotic individuals would suffer less from unnecessary tension operating on lower levels, and from other negative dynamisms related to psychoneuroses and enhanced by wrong attitudes in relation to psychoneurotics. The new approach would permit to accelerate individual development and its greater fullness, and in consequence would give the society the advantage of making use of the original and creative aspects related to nervousness and psychoneuroses.
219
CHAPTER XII
THEORIES OF NEUROSIS AND THEORIES OF DEVELOPMENT
In this chapter we shall give a comparative overview of different conceptions of psychoneurosis and contrast them with the developmental approach offered by the theory of positive disintegration.
1 Psychoneurosis as a Prelude to Mental Illness
J. Hughlings Jackson (1958) and the neo-Jacksonian schools represent the opinion that psychoneurotic syndromes are manifestations of the initial phase of dissolution of psychic activities, and that the evolution of these psychoneurotic dynamisms leads to serious mental illness. The theory of positive disintegration is directly opposed to this view (Dąbrowski, 1964; Dąbrowski, 1967; Dąbrowski, Kawczak, and Piechowski, 1970). Nervousness and psychoneurosis, in our opinion, are signs of the beginning or already advancing process of positive development. Intense psychoneurotic processes are especially characteristic of accelerated development in its course towards the formation of personality. According to our theory accelerated psychic development is actually impossible without transition through processes of nervousness and psychoneuroses, without external and internal conflicts, without maladjustment to actual conditions in order to achieve adjustment to a higher level of values (to what “ought to be”), and without conflicts with lower level realities as a result of spontaneous or deliberate choice to strengthen the bond with reality of higher level. It was shown in Chapter 7, section 4, that, if anything, psychoneuroses prevent the
220
development of mental breakdown, or if such occurs it is thanks to the psychoneurotic dynamisms that recovery is possible.
2. Psychoneurosis as an Organic Disorder
The theory of positive disintegration is also opposed to that conception represented, by Maudsley (1868; 1873), Sargent and Slater (1954) and others, who hold that psychoneuroses are disorders of an organic nature and the discovery of the organic and biochemical defects is the goal of scientific and clinical psychiatric research.
We think that the fact that some internal somatic or neurological troubles are related to some symptoms similar to those of psychoneuroses is not sufficient justification for the proposition. Of somatic etiology in the majority of psychoneuroses.
The somatic correlates of neuroses and psychoneuroses are discussed in more detail in Chapters 3 and 4.
3. Regression and Emotional Immaturity as the Source of Psychoneurosis
In relation to the schools or research groups which consider emotional immaturity as the fundamental element of psychoneuroses (Masserman, 1943; Mazurkiewicz, 1950; Zajaczkowski, 1961) the theory of positive disintegration gives room to the view that so-called “psychic infantilism” is not a homogeneous phenomenon (Dąbrowski, 1967). Furthermore, in our view several of the features or symptoms of such infantilism constitute positive developmental properties, or possibilities of positive development, which are also inherent in psychoneuroses with structures and functions of a very high level of growth and creative potential. Such traits as absence of automatism, some elements of magical and animistic thinking, creative aptitudes, sincerity, spontaneity, capacity for feelings of wonder, or amazement and anxiety with respect to reality are all characteristic of some infantile types, of accelerated development, as well as of high levels of interneurotic and intraneurotic functions (see Chapter 5, Section 1 (6), and Chapter 10).
The so-called positive regression, characteristic of sensitive and able individuals, and also of nervous and neurotic indivi-
221
duals, is the expression of the need to become saturated with experiences of great impact and tension, harmonizing the rich inherited psychic endowment in preparation before various conflicts in the external life. This, then, reflects a tendency to prepare and to strengthen the inner psychic milieu to face new trials [see Chapter 5, Section 1 (5)].
4. Psychoneurosis as a Disorder of the Reality Function
In contrast with the school of Pierre Janet we have a multilevel view of the reality function.
Janet (1926) considered neuroses as definite psychic diseases, without discerning in psychoneurotic processes any elements of positive potential for man’s psychic growth. He regarded the symptoms of contemplative or ecstatic elevation as sick or abnormal [see Chapter 8, Section 5 (5)]. However, the one element common to both theories is the fact that Janet regarded, as we do, psychoneuroses to be disturbances of psychological functioning, without the consequences of a permanent structural damage (see Chapter 3, Sections 1 and 2).
Janet (1926) was concerned primarily with two forms of neuroses: psychasthenia and hysteria. The first is connected with disturbances of the will and of the reality function and is manifested by conditions of depression and associated anxiety; the second is manifested by disturbances in perception and personality structure.
Psychasthenia is the syndrome which Janet was first to differentiate, describe and interpret. Psychasthenia is manifested by the weakening of the reality function, which is the highest function in our hierarchy of mental functions. A psychasthenic may solve a difficult mathematical problem, but it will be difficult for him to keep an account of personal income and expenditure, he may be qualified and could win an important position, but will not make the final steps to get it. A disturbed reality function in psychasthenics is either connected to other functions, or separated from them, and may raise or lower them in the hierarchy of mental functions.
The combination, and synthesis of mental functions (unification, concentration) with many manifestations of
222
consciousness is manifested in psychological tension. The lowering of that tension explains the characteristics of psychasthenic depression states, feelings of insecurity in one’s own behavior, disturbances in intellectual, volitional, or affective powers. Some misfortune causes a lowering of mental functions and the disengagement of a certain complex from among them. This complex, following an initial condition of functional dispersion, assumes a systematic form, wherein instead of psychomotor overexcitability there appears an obsessive thought, a phobia, etc. This development appears to result from a desire to substitute general psychical insufficiency by actions apparently better adjusted.
Psychasthenics show an inability for action, and this weakness takes on several pathological forms in which they may delight insofar as they provide justification of their inactivity.
Hysteria, recording to Janet (1920), is a form of mental depression and is characterized by a narrowing of the field of consciousness by dissociation of functional systems. These functional systems when normally unified, make up the whole personality. According to Janet hysteria is a disease of personality synthesis. Janet recognized the serious, but not exclusive, role of suggestion in the development of hysterical symptoms, judging that these symptoms may also develop as a result of emotional conditions remaining outside suggestion. Janet was also of the opinion that, in certain cases, an hysterical condition may develop when the individual thinks the same thoughts for an excessive length of time.
However, he maintained that a majority of hysterical disturbances are produced sub-consciously, independently of the will. Janet’s view was that the narrowing of the field of consciousness consists of mental weakness and is manifested by the reduction of the number of psychical phenomena which may be simultaneously combined in the same consciousness.
In his later years Janet emphasized the concept of “forces” in psychology, and the changes in hierarchy and combination of tendencies—all of which is summarized in the concept of psychological tension. A high psychological tension provides complete activation; a low tension is responsible for lower tendencies, lesser activation. When the psychological tension
223
is decreased, pathological symptoms occur, such as obsessional hysterical thoughts, dissociation, narrowing of consciousness.. The background for these symptoms is provided by hereditary weakness of psychological tension, and also by physical and nervous strain. The weakening of the reality function, is also manifested among psychasthenics.
In my view the reality function organizes drives and tendencies in their adjustment to the environment. The reality function will necessarily be disturbed during the individual’s growth. Furthermore, the reality function corresponds to a certain level which must be changed, loosened, or disintegrated in order to allow another reality function to develop, at a different level; at this new level it must acquire, as it were, new coordinating elements. In my opinion (Dąbrowski, 1963), the reality function is a function of a disposing and directing center and is constantly striving towards higher levels in phylogenetic and ontogenetic development.
Among individuals gifted with the capacity for mental growth, especially among the most outstanding, there occur fundamental changes in the structure and localization of the disposing and directing center, as in the basic personality change exemplified by St. Augustine or Dawid; therefore, their reality function was also transformed (Dąbrowski, 1967).
Of course there are people who have little or no capacity for growth; they realize only their genotype, without any sense of conscious self-development.
In the eyes of a large sociological group which is uniform as far as their level of development is concerned (i.e. they are consolidated by common habits, levels of motivation, or vices) other groups possessing a different level of attributes will appear as groups of unreal or impractical people. An inventor of things which are not immediately of practical value will be considered unrealistic despite the great value the invention may have in the future. Unselfishness, asceticism, sacrifice, will appear for many to be only a sign of a lack of realism, day-dreaming, fantasy, or even mental disease. This is the common attitude of a majority of people and is even an opinion shared by many so-called experts on the problems of psychoneurotic individuals.
224
The psychasthenic who gives others many a fertile idea, who will create an important work of art or science but fails to publish is said to be exhibiting an impractical attitude and will likely be judged as having no sense of reality. An individual living in the world of retrospection and prospection, who cannot and would not adapt himself to the actual daily reality, will be considered an unrealistic man, or one disturbed in his reality function. A person who values his own inner independence more than he does adaptation to a mediocre level of a milieu will be judged an unrealistic politician or moralist.
However, each of those individuals may present a highly developed sense of “reality,” with the provision that this sense expresses the development of a reality function of a different level than is accessible to the majority. Among those who are gifted with a high enough reality function, real value may be given to sacrifice, unselfishness, or asceticism.
It is necessary to further supplement the above considerations. The weakening of the reality function may concern not only those individuals who have established their disposing and directing center at a high level, but also those who, having a reasoning capacity and a fair ability to understand and appreciate reality, have no desire to adjust themselves to it. It is of such individuals, among others, that we have spoken above. We are not concerned here, on the other hand, with mentally retarded people who are either incapable of maintaining a reality function on any but the lowest level, or who make only partial use of it. Another qualification: a developing individual is not growing simultaneously in all areas of his personality. In certain periods of life development may be centered in one area, leaving other areas unaffected. This applies to a large number of people of accelerated, albeit one-sided development, and psychoneurotics are among them. “Planned” development may last all one’s life. That is why the consideration of the reality function as a synthesis of the whole personality with all its elements, is an abstract problem. Thus, it is difficult to agree with Janet’s (1926) definition of “reality function.”
225
5. Subconscious and Unconscious versus Conscious Conflict in the Genesis of Psychoneurosis
In comparison with Freud’s theory and the orthodox psychoanalytic school, the theory of positive disintegration also accepts—but to a lesser degree—the role of subconscious dynamisms in both normal and pathological processes of human life. Our theory stresses the great importance of inner conflicts in the formation of psychic structures and dynamisms, but we place the emphasis on the positive side of those conflicts.
In Freud’s theory (1949) of neuroses an important place is given to the structure and dynamisms of childhood drives. According to this viewpoint a child’s behavior follows a pleasure principle (Lustprinzip). The motive power of this action is “libido,” or that energy which is expressed in sexual drive. A sexual symptom is, according to Freud, everything that originates in the sexual drive. Normal and pathological psychical events may have sexual coloring, even though their nature appears to have no direct relation to sex. This drive, it is claimed, is not +peculiar to puberty but can also be found in a newborn baby.
During the so-called “latency” period—usually between the ages of 6 and 8—most events from the earlier period of a child’s life are forgotten as a result of repression or displacement into the unconscious. Psychological, but especially educational influences are responsible for the repression. Often libido is abnormally developed, due to some constitutional elements, excessive inhibition, faulty education, or strong emotions. It remains fixed in certain childish traits which are not eliminated and are not adjusted to social life.
With respect to repression of conscious events, Freud stated that they may be forced into the unconscious, with much of their content never reaching consciousness. The cause of various unconscious processes is the contradictory action of two opposite desires (or purposes), one of which is apparent and the other hidden and unconscious. The sub conscious and the unconscious processes are expressed in dreams often in symbolic form, acceptable to the censor or “guard” who watches, as it were, on the borderlines of con-
226
sciousness. This censor, according to Freud, is a function of the “ego” (Ich), or our personal consciousness, developed by the instinct of self-preservation. Corresponding to the conscious “ego” is the dark and primitive aspect of our personality, the “id” (Es). In the subconscious there is also the “super-ego” (fiber-Ich). “Superego” is the subconscious representative of our relations with our parents, it represents the internalization of parental prohibitions, expressing the need for penance and punishment; it is the source of religious and social sentiments.
Neuroses, according to Freud, result from the conflicts between the “ego” and the “id.” The “ego” depends on reality and in trying to adjust to reality, represses part of the “id”; the “ego” is then transferred from the pleasure principle to the reality principle. The action of the pleasure principle is thereby thwarted. This results in an improper development.
Freud divides neuroses into two types:
l. actual neuroses; neurasthenia, anxiety neurosis and hypochondria.
2. psychoneuroses; conversion hysteria, anxiety hysteria, and obsessive neurosis
The etiology of the first group is to be sought in physical factors, the second—in psychic factors. In the first type, pathological causes and the symptoms appear at the same time; the earliest cause of the second type is to be sought in childhood. In the first type analysis may not prove the existence of any psychic trauma, in the second one it does, as a rule.
Psychoneuroses were also called “transference neuroses” (Ubertragungsneurosen), and said to result from a transfer of inimical or pleasant feelings and drives of the patient, from the people closest to the patient in childhood (mother, father, sister, etc.), to the people (doctor, teacher, spouse, friend) in the actual situation in the present.
The conflict between the “ego” and the “id” results, according to Freud (1943) in neurosis. From the point of view of personality development, however, this is not necessarily to be avoided. A psychoneurosis often appears necessary in development and is gradually overcome with the progress of autopsychotherapy.
227
Conscious sublimation and transformation of lower drives is not a stage which is arrived at without intermediate stages of conflicts, repressions and failures. True enough, neurosis may be explained, as pointed out by Freud, through conflict of contrary psychic forces, but the outline of the conflict and its significance in personal development is completely different in the theory of positive disintegration than in Freud’s theory. It is true that excessive inhibition may lead to negative regression, but inhibition may also lead to higher forms of development even though it is not completely conscious. In the formation and development of neuroses several different factors contribute, and the sexual drive is not necessarily the only nor the strongest one. Bleuler (1911) remarks quite correctly that nervousness cannot be identified with sexuality. Rather, it may be connected to a conflicting attitude with respect to sexuality.
Furthermore in many neurotic syndromes, whether hysterical, anxiety, or psychasthenia, the sexual element plays a secondary role or is negligible. Good examples are the first three cases given in Chapter 2.
Freud’s interpretation of dreams, as understood by Jones (1920), is not correct in saying that the only material that is symbolized is that which has been repressed, and only that which is repressed has a reed for a symbol. Much of the inner subconscious or unconscious content is not revealed, not because it is being opposed by consciousness, but often because we either do not feel the need, or we lack the ability to transform and understand subconscious experiences, past or present. Daydreaming, fantasy, tendencies for mystical experience, are connected consciously or unconsciously with prospective tendencies slowly grasping the new, still uncontrolled reality.
It appears that Freud as well as his followers have failed to appreciate the positive value of psychoneurotic conflicts of a multilevel character. They attempted to reduce a large developmental phenomenon to the narrow field of those disorders which are related—in some sense—to typological traits. It becomes understandable that many individuals are attracted to psychoanalysis, not so much to seek a cure through sublimation of their drives, but often rather as an expression of their desire to discuss,
228
discover, and experience problems of a sexual nature, which never cease to excite them.
Freud’s penetrating analysis of neurotic and psychoneurotic complexes (conflict mechanisms, repressions, conflicts between conscious and subconscious processes, structure and personality dynamics), and his insights were, it seems to me, permeated with pansexualism, having a dominance of the “libido” principle without properly appreciating psychoneurotic processes in personality development, and without noticing the role of “developmental drive” in both normal life and in processes which are called “pathological.”
Basic differences between the two theories may be briefly outlined as follows:
(a) Psychoanalytic theory does not recognize to a sufficient degree the multilevel aspect of psychic events. There are no notions of a hierarchical inner milieu whose nuclei could be discerned in an early manifested developmental potential. The hierarchy of “id,” “ego” and “superego” is restricted to the sexual instinct alone even if taken in its broadest sense. The psychoanalytic theory does not recognize the problem of multilevelness of emotional and instinctive functions in the sense of their potential and their development. It does not distinguish different levels of defense mechanisms. Some defense mechanisms are in the service of higher developmental dynamisms in order to protect their evolution in conflicts with lower dynamisms (Chapter 6, Section 4). Such conception involves the whole domain of growth and development, not just pathological processes.
The psychoanalytic theory also does not take into account the multilevel nature of psychoneurotic processes, internal conflicts, creativity or sublimation (especially the loss, elimination or irreversible transformation of lower instinctual levels).
(b) In keeping with the evolutionary conceptions developed by John Hughlings Jackson the theory of positive disintegration represents a developmental point of view in relation to “life difficulties,” nervousness and psychoneuroses. In the “normal”—but especially in the accelerated—process
229
of development of mental functions different kinds of disorders occur. In the vast majority of cases these disorders are both a necessary and a positive phenomenon. In the development of mental functions from their primitive to more complex forms, from their automatic, unconscious (or subconscious) to conscious forms, there is almost always certain temporary disorganization, nervousness, psychoneurosis, expressed by internal and external conflicts, depressions, anxieties, suffering, positive maladjustment, etc. These problems are either omitted in psychoanalytic theories or else are treated only in their negative, destructive, pathological aspect. I refer here primarily to defensive mechanisms, repressions, conflicts, fears and other neurotic and psychoneurotic symptoms.
I The problem of the “third factor.” The psychoanalytic theory sees the source of human development only m terms of innate and environmental factors. It stipulates that the conscious, but even more the sub- and unconscious mutual interaction of the individual with his environment is the main object of psychoanalytic inquiry and therapy Such is the position of both the orthodox psychoanalytic school and all neo-psychoanalytic developments. On the other hand, the theory of positive disintegration postulates the existence of a “third factor,” whose role lies in making conscious choices through the affirmation or negation of certain values, trends, behavior, people, etc. These choices apply both to the inner milieu and to the external environment. The activity of the third factor transcends the determining influences of heredity and of the environment as well (Dąbrowski, Kawczak, and Piechowski, 1970). The “third factor” is the dynamic agent of autonomous, conscious, self-determined personal growth. The “third factor” may become the main dynamism steering personal development, which is observed both in clinical data and numerous examples from biographies of historical personalities. In many patients we can differentiate very clearly the genesis and development of this factor. In higher forms of psychasthenia, psychoneurotic anxiety, depression and psychoneurotic infantilism we clearly observe the
230
increasing action of affirmation or negation and choice in relation to the individual’s own tendencies and in relation to stimuli from the external environment. In longitudinal studies of such patients, we see very strong symptoms of the development of this third factor. In many patients we observe very clearly at first the lack or weak expression of this factor and in subsequent periods, the appearance and clear action of this dynamism (Dąbrowski, Kawczak and Piechowski, 1970).
6. Adler: Asocial Compensation for Feelings of Inferiority
The problem of inferiority feelings was introduced into the diagnosis of psychic disturbances by Alfred Adler (1927). In Adler’s individual psychology a considerable role is given to the analysis of a supposed dominating tendency in an individual life, the so-called lifestyle (Lebensleitlinie), which derives from the individual’s goal in life. Among all neurotics this goal may be traced according to Adler, as a drive for superiority (Uberlegenheit) through the will to power (Will zur Macht) or the will to be a man (Mannseinwollen). One of the conditions (rot necessarily sine qua non) in the formation of nervousness and neuroses is an impairment of some organs (Organminderwertigkeit), e.g. in the circulatory, urogenital, or digestive system. Adler gives this definition to the “impaired organ”: “It is an organ unformed, underdeveloped at least partially, or arrested in its development” (Adler, 1917; Adler, 1924).
Against this background of a more or less conscious or unconscious physical inferiority there develops the feeling of inferiority and an aspiration for psychical compensation. The above process, which is quite clear among neurotics, is a universal phenomenon among children for whom the feeling of weakness is as common as is the need to arrive at some feeling of strength and status. Now, the awareness a person has of his individual shortcomings does not necessarily lead-according to Adler—to the discovery of an appropriate method leading to their compensation. That is why compensation may be effected either in a socially acceptable or asocial manner depending on the milieu.
231
Neurosis occurs—according to Adler (1928)—as a result of using improper means for attaining the end of becoming superior to others.
Among children, the first instance of either social or asocial compensation is through the parents, especially the mother. Since a child is so dependent on parents and elders, a feeding of a certain void or need is formed. To compensate for that need, or in general any deficiency feeling, a fiction is created which is personified in the father, teacher, or a male hero from a novel. A scheme is formed associating the concept of superiority with that of manliness, and the concept of inferiority with womanliness. From the very roots of the conviction of the superiority of a man there springs the so-called masculine protest.
Those who cannot attain the realization of their desires may try to achieve superiority by way of limitless submission (masochism). This is the so-called transformation of form for handling the task of removing the sense of inferiority. Very submissive individuals often still want to be the center of attention and interest.
The Oedipus complex loses its sexual significance, in Adler’s view, and expresses rather a desire to influence the father and mother.
Dreams are a preparation, an unsystematic test, as it were, of the life-style. They support the drive for security, and are helpful in maintaining the desire for power and feeling of superiority. The weakening of inhibition which occurs in sleep and day-dreaming makes it easier to live a fictional life. In night dreams a feeling of inferiority is expressed together with a tendency for its compensation. According to Adler, he who dreams is he who is not sure of himself. There is no dynamic difference between the conscious and the unconscious; their aim is the same.
Analogous to Freud’s pair of contrary principles of pleasure and reality, we find in Adlerian theory the principle of conformity or the social principle, which is opposed to the “will to power” built on the basis of inferiority feeling.
In spite of a somewhat detailed analysis of “impaired organs”
232
Adler (1924) ascribed a very minor role to heredity. A child’s psyche constitutes the material for the development of unlimited possibilities which are realized depending on the influences of the milieu. Adler recognized physical heredity, but not psychical heredity. In his view, the determinant of proper or improper development is the absence or presence of dysfunctions of organs or systems of organs. These dysfunctions, or improper social interaction, determine asocial compensation of feelings of inferiority and lead to an improper life course. A fundamental difference between both theories rests in the influence attributed by our theory to positive hereditary endowment, and to the role of authentic, autonomous factors in the development of man. These are formed as the individual development proceeds and are closely connected with psychoneurotic dynamisms. As human growth proceeds, these dynamisms carry out the work of deciding what is to be accepted and what is to be rejected in the psychological make-up of the individual as well as in his external environment. While acknowledging the role of feelings of inferiority with respect to the external environment, our theory considers the feelings of inferiority with respect to oneself to be of equal, if not greater, importance and to participate, along with other dynamisms of the inner psychic milieu, in human development. Sin, according to Adler, is a reaction to a deviation from the “straight line” of life. In my opinion the feeling of sin, together with feelings of inferiority toward one-self, guilt feelings, discontent with oneself, represent clear dynamisms of positive development. An individual who does not feel “sin” often presents psychopathic or even criminal tendencies.
According to C. Macfie Campbell (1933) a feeling of inferiority is to be found at the basis of our best efforts and it may be that no great achievements are possible without some contribution from this feeling. The feeling of inferiority together with its compensation by creative efforts is well accepted in all major educational systems as well as in all great religions.
We feel that it is necessary to distinguish between feeling of inferiority with respect to others, from that with respect to oneself. A feeling of inferiority towards others is expressed in an overestimation of strength, fitness, knowledge or wealth of
233
others. It is a feeling invoked, as it were, through external experiences. It is connected with submissiveness on one hand, and with jealousy on the other, and may find expression in a tendency towards measuring up to others and attempting to get on top even with aggression. The feeling of inferiority with respect to oneself, or to one’s own potential, on the other hand, is a feeling connected with the genesis and development of an inner psychic milieu. This feeling denotes the capacity for distinction between higher and lower levels and the feeling, of relative closeness to or distance from one’s own “ego.” It denotes also, an occasional submission of the disposing and directing center to the action of lower dynamisms, and it denotes also the inevitability of inner conflicts.
Just as it is characteristic of those possessing the feeling of inferiority towards the external world to have a tendency to overcome it through aggression, envy, or jealousy, it is characteristic for one with inferiority towards oneself to express feelings of shame, dissatisfaction with oneself, guilt, an attitude of humility, and conflict with one’s own lower dynamisms (i.e. primitive levels of basic drives).
The latter type of inferiority feeling is very commonly observed in cases of psychoneuroses, especially in obsessional neuroses, anxiety neuroses, depression;, and psychasthenia—that is to say—in all those neuroses which are characteristic of the stage of multilevel disintegration.
The mechanisms involved in the development of feelings of inferiority in some psychoneuroses are analogous to those active in “normal” individuals who have discovered their ideal for development, and an ideal of moral perfection by subjugation or even elimination of lower drive responses. The only difference is that in the latter case conflict responses are less visible and may be controlled with more facility, thereby causing no need for the intervention of a physician. An inferiority feeling towards oneself is, therefore, one of the developmental mechanisms active in psychoneuroses. This viewpoint is contrary to that of Adler (1927) who recognized only the feelings of inferiority with respect to the external milieu. The feeling of inferiority towards oneself is a dynamism especially strong among indivi-
234
duals of a high level of development and occurs more frequently among adults than children.
Adler described not only the asocial compensatory mechanisms but also socially positive dynamisms of compensation and sublimation. The latter can be regarded as a system of values for education (Adler, 1938).
7. Jung’s Conception of Psychoneurosis and Development
There is some similarity between Jung’s theory (Jung, 1933) and the theory of positive disintegration. According to Jung, neuropathy is a special case of a man lacking unity within himself. The causes of inner disharmony are attributed to certain deviations in human growth from a primitive to a cultured condition, due to weakening of some instincts with concomitant strengthening of others (for example, hunger instinct is weakened or decreases in importance, to the greater gain of the sexual instinct, as a result of conditions wherein direct striving for food is no longer vital. According to Jung, neurosis resulted from an unsuccessful attempt at solution of vital human problems within oneself. Thus, neuroses are not only results of some pathological causes, but are expressive also of an attempt at a new synthesis of inner contradictions.
The theory of positive disintegration does not recognize psychoneuroses as expressive of developmental deviation, but views them as appropriate and even accelerated forms for human development in its positive drive from a primitive to a cultured condition. “Disagreement with oneself,” which is emphasized by Jung, we view as a background which is fundamental to the formation and development of the inner psychic milieu, and thus, to the development of man. On the other hand, both theories are in agreement in proposing that psychoneurotic symptoms and dynamisms are expressive of attempts at a new synthesis of internal conflicts.
Jung (1921) distinguished two basic psychological types: the extravert and the introvert. The extravert type is characterized by a positive attitude towards objects and events. An individual of this type thinks, feels and acts in a way which is straightforward and understandable to his environment. He is practical,
235
adjusts easily to others, does not like being alone. His criteria of values are socially established norms. The introvert type is characterized by a negative attitude towards objects and events. His thoughts, feelings and actions show that the factor determining his behavior is the individual himself. An individual of the introvert type has more difficulty in adapting to his environment, to changed conditions, does not trust others, is critical towards accepted norms. He retires into his own inner world.
One rarely encounters a pure extravert or a pure introvert. Normally any individual is a mixed type with a predominance of extraversion or introversion.
For both introverts and extraverts Jung distinguished four sub-types: thinking, feeling (emotion as a function of valuation) sensing (Empfindung—perception occurs through the senses), and intuiting (unconscious or instinctive perception).
Thinking and feeling are rational functions while sensing (Empfindung) and intuition are irrational functions. There are four possible combinations of these functions in each of the two basic types. For instance when thinking and intuition are combined in an introvert type this often is expressed in abilities towards philosophy. Intuitive extroverted individuals tend to love to travel.
Extraverts always possess some introvert traits although to a lesser degree and expressed subconsciously. Likewise introverts have some extravert traits. In each pair of rational and irrational functioning one is dominant and the other is sub-dominant and subconscious. For instance in the feeling type thinking will occupy a lower position while in a sensing type intuition will occupy a lower position.
Normally an individual of a given type (extravert or introvert) with one dominant pair of functions (one rational and one irrational) will exist in certain balance with the opposite aspect of his psychological constitution. The opposite aspect remains unconscious but the individual’s psyche is flexible to the extent that he can at times accommodate his subconscious functions. When the balance is too much into one direction and a concrete situation requires acting according to the opposite aspect of the psyche then this demand, for which the indivi-
236
dual is not prepared, leads to psychic disorders. Thus extroverts usually develop hysterical disorders. In the initial stage the normal and dominant aspects are strengthened (great desire to center the environment’s interest on oneself, great susceptibility to environmental influence and the like). This is subsequently complicated by a compensating reaction of the subconscious which directs the excess of extraverted energy inwards to inner problems. As a result there may be certain physical disturbances. Extravert feeling types under conditions demanding: thinking, while their thinking is usually much suppressed, develop perseverations of thoughts. In extravert sensing types arise states of anxiety, perseverations and special phobias, as an expression of feelings and thoughts suddenly demanding, release from the subconscious. Extravert intuitive types develop similar conditions under the stress of grave experiences. In introverted types excessive turning away of interests from the objects of the external world creates resistance, life of the external world becomes more and more attractive. Such individuals become affectively excitable and easily subject to fatigue. Psychasthenia with states of anxiety is their characteristic psychoneurotic disorder. Objects, the external world, normal preoccupations evoke inexplicable fears. It appears to them that the object has some atavistic power; they fear new objects and new situations; hence nostalgia for solitude and silence (lonely island). In introverted thinking types the loss of equilibrium is expressed in a warfare of opposing tendencies: absoluteness and inconsiderateness in: relation to others on the one hand, and on the other—fears and affective overexcitability. In introverted feeling types we encounter as the most severe disorder neurasthenia as a consequence of a conflict between excess of affect and intellectual needs (on the one hand fearfulness and inhibition, on the other creation of systems of thought, tendency toward polemic and argumentation). Both irrational introvert types (intuitive and sensing) as their typical disorder develop perseverations, of images and thoughts as a reaction to their extreme ability for perception and fantasy.
It can be seen from the above short presentation that for Jung neuropathy is a special case of man disunited with himself
237
(Jung, 1926, p. 30). The causes of this disunion exist as a result of certain deviations in the progress of mankind from primitive forms of existence to the formation of culture. In this progress certain instincts lost their power to other instincts, e.g. the fact that there is no need to be directly involved in securing food the driving power of hunger is much weaker while the sexual drive became stronger.
According to Jung neurosis is an expression of a failed attempt to find within oneself the solution to a general problem (Jung, 1926). The manifestations of neurosis are not only the consequence of certain observable causes (sexual infantilism or will to power) but also of an attempt to create a new synthesis of life from existing antinomies. If the activity in one direction is too strong and if there is an insurmountable difficulty, then there comes a regression into the deep unconscious strata of personality. It is than that forces are manifested which had no access to consciousness or only to a very limited degree, e.g. aggressiveness and despotism provoke their sub-conscious complements in the form of fears; asceticism and severity evoke passion. The unconscious processes are expressed in a primitive form because the unconscious is always more primitive (by being older) than consciousness (Corrie and Jung, 1928).
On the basis of dream analysis and free association Jung came to the conclusion that the symbolic form of the unconscious contains an archaic content—primitive images and feelings common to all mankind such as primitive and I explanations of the phenomena of nature through myths of the sun, moon, birth of a god, fear of objects and phenomena. Modern man, whether normal or a neuropath, has these images and contents appear in his dreams at night and in his waking dreams, except that the neuropath experiences them more vividly and with greater intensity. These archaic remnants appearing in unconscious processes in symbolic form Jung called archetypes (Jung, 1926). This is the collective unconscious, so termed by Jung because of its collective character common to all mankind from time immemorial.
The collective unconscious is a different concept than the individual subconscious, which carries contents forgotten or
238
suppressed from the personal experiences of the individual. In dreams both the unconscious and the subconscious contents appear in complexes, i.e. contents emotionally colored [the content is as if made of two parts: primary core component and numerous secondary associations (Adler, 1927: 1930). The deeper the stratum of the dream the more collective is its meaning.
For Freud a symbol was a static image, for Jung it is a dynamic experience (Jung, 1928). From consciousness we move to our personal subconscious as its hidden and lower complement, and further to the collective unconscious as the deepest stratum. It is there that we ultimately find the sources of conflicts created by the cultural conditions of our age, by violation of nature’s laws, by suppression of the unconscious by the conscious. These conflicts appear as neuroses.
To find the sources of conflict and neurosis Jung used the following methods:
1 Association—more important complexes are revealed by providing the patient with words as stimuli to which he responds. The list of words is specially compiled to fit the patient.
2. Hypnotic suggestion—symptoms are analyzed in the light of memories revealed under hypnosis, which may be the basis of the neurotic conflict.
3. Anamnesis—analysis of the patient’s past in order to arrive at a genetic reconstruction of the neurosis.
4. Analysis of the unconscious (dreams, free association, slips of tongue, etc.) carried out after the conscious contents have been analyzed.
These methods are different from Freudian psychoanalysis which is in essence an analysis of the sexual life and its implications for the individual. The essential trait of Jung’s approach is an analysis of the unconscious without the initial assumption specifying what contents are to be found.
Jung’s theory in many ways enriches Freud’s theory at the same time taking away it’s pansexual character. It is to Jung’s great merit that he drew attention to the role of artistic,
239
scientific and religious values in the life of both the neuropathic and the normal person. He showed the great significance of these values in neurotic conflicts. He proved that some of them are primeval and act from birth (Nachmannsohn, 1933). The conflicts of these forces represented by values mentioned above play a big role in the life of the unconscious, they appear in dreams in symbolic form, and, therefore, need to be taken into account in the analysis of symbols.
Jung’s approach opens a much wider basis for the analysis of dreams than was available in psychoanalysis before him. A symbol does not necessarily represent something that was suppressed but rather enables us to understand the future psychic development of an individual. I quite agree with Jung that to take into account life goal as a dynamic psychological factor is indispensable for the understanding of the form, development and resolution of psychic conflicts. By comparison, to be limited only to analytic methods and to the search for causes is indeed to be limited.
The idea and the development by Jung of the method of association is undoubtedly one of the great contributions to psychiatry. However, his detailed typology has more defects than virtues which is a consequence of the fact that the question of typology has always eluded successful systematization. There is more practical value to the distinction of the two basic types (the extravert and the introvert) justified by factual evidence. The theory of archetypes and the collective unconscious are full of hypothetical assumptions, vagueness, and do not appear to be of much practical significance.
The lack of a clear distinction between the conscious and the unconscious level and of different levels of mental functions appears to me to deprive Jung’s theory of an understanding of the more valuable syndromes and dynamisms in psychoneuroses. The lack of a clearly elaborated multilevelness of emotional and instinctive functions left Jung without a basis to clearly delineate the developmental path of man in relation to all basic functions (intellectual, emotional and instinctive) from the unconscious to the conscious, and from the conscious to the superconscious
240
This path of development is a path of transformation of archetypes into “neotypes,” of individual unconscious into individual superconscious v. which contains all the elements of human psychic structure. Naturally such achievements are paid for with suffering, disintegration and psychoneurosis.
The structures of the collective unconscious and of the individual subconscious have to be transcended if one is to move on the way to consciousness and superconsciousness, and for this reason an equilibrium between the two levels cannot exist. The equilibrium can be achieved only when the individual attains the higher level of consciousness and super-consciousness, which controls its lower levels. The way to such an equilibrium leads through disintegration and psychoneurosis.
Jung’s conception of the relation between suffering, pain, joy, individual ecstasy and identification with these states in others and in relation to the whole world is not quite clear. It seems as if Jung did not offer attempts of solving the difficulty of preserving and deepening the relation between “I” and “Thou” without a loss to each one involved. This demand of transforming individual pain, suffering and joy into universal and cosmic suffering and joy gives his theories a monistic flavor This, however, is often unacceptable to many psychoneurotic patients endowed with the capacity for accelerated development.
All these Jungian conceptions indicate lack of a unified approach to psychoneurosis as a positive process of development. This is well exemplified in his following statement: “Neurosis is integrally bound up with the problem of our time and actually demonstrates the unsuccessful effort of the individual to solve in himself what is essentially a universal problem. Neurosis is the division with the self” (Jung, 1961, p. 76). We cannot agree, however, that neurosis is an “unsuccessful effort.” The fact that psychoneurosis is an expression of division within the self is a positive phenomenon and here we agree with Jung completely. Jung himself adds sometimes remarks which agree with our theory: “Neurosis is by no means only negative; it is also positive”; “every illness is
241
a purgatorial fire” (quoted after Paracelsus, Jung, 1961 pp. 84 and 254).
Jung’s comments that a psychotherapist cannot be a psychoneurotic if he is to be an effective therapist, do not appear entirely justified. What needs to be specified is that the psychotherapist must have achieved a higher level of psychoneurotic processes, or that he must have gone in his development beyond psychoneurotic experiences. Without that he could not be a good psychotherapist.
Jung was not a child psychopathologist, hence his theory has little to offer toward problems of nervousness in children and adolescents. A theory of an overgrowth of conscious factors in personality and of the suppression of its lower unconscious components cannot be applied to a child who has not yet been formed that way. Nevertheless it seems to me that Jung did not appreciate the significance of his distinction of the two essential types for the psychological prophylaxis of children’s development.
* * *
Jung divided therapy into four stages: insight, explanation, education, and transformation (Nachmannsohn, 1933). The first stage is common to all schools of psychoanalysis because it follows from the principle that it is absolutely necessary to explain those mysteries of the unconscious which are harmful for the individual and for the society. Catharsis serves as a means of removing the excessive feeling of sin and guilt which usually arises from lack of knowledge and sense of mystery in the area of instincts. Only in rare cases insight alone can effect a cure of a neurosis. Thus it becomes important to lead the patient to the second stage which is explanation on the basis of analysis of his dreams and associations of the dynamics of his individual and collective unconscious and recognition of the sources of “transference.” When the patient can differentiate between what is his self and what is collective, he can then channel his energy to proper ways of handling his life. This is a purification of consciousness by separating from it the contents which are mythical and collective.
242
It is on this level that Jung begins the work of transforming the patient into a social being. The therapeutic influence is here identical with Adler’s method of education, except that Jung introduces the fourth stage. At this time the constellation of the patient’s forces is transformed in agreement with his psychological type and the direction of his tendencies (teleological principle). To be able to realize such tedious and responsible tasks the therapist has to test this method on himself, and also he has to be of high moral standing.
The Jungian method is not applied in its full extent to children and adolescents because the question of the collective unconscious contents does not play such an important role as in adults. The analysis of dreams is usually dispensed with because subconscious themes should not be suggested to children since this would make them inappropriately curious and could cause a precautious development of self-awareness (Jung, 1928).
The principles of Jung’s therapeutic education are not clear. The theoretical vagueness of the problem of the collective unconscious, which Jung considered in therapy necessary and important to separate and differentiate from personality, does not help one to be convinced of its therapeutic value. The interpretation of the unconscious contents must necessarily remain unclear and does not give a basis for systematic psychotherapy. Nevertheless, one must assume that Jung’s extensive psychological knowledge and his profound insight enhanced his effectiveness as a therapist.
7. Karen Horney: Psychoneurosis as a Childhood Trauma
The school of Karen Homey (1937)—in accord with, the orthodox Freudian school—looks at psychoneuroses, especially anxiety psychoneuroses, as resulting exclusively from frustration of early childhood. The anxiety is brought about by stressful events in the environment. There are, however, many examples of children brought up in the best of environments, under wise educational influence in both early and later childhood, who still manifest increased psychic excitabilities of various kinds, including fears, anxiety states, inhibitions, obsessions, etc.
243
Horney’s observation that many psychoneurotics develop their own “idealized neurotic self-image” is correct, but one has to consider that this image is often positive and related to an accelerated growth of the individual. Such growth occurs with the participation of “psychoneurotic” dynamisms like internal conflicts, feelings of inferiority in regard to oneself, positive maladjustment, personality ideal (autonomous rather than imitative). One should also keep in mind that stress and frustration are influential not only when occurring in childhood but may appear with equal force in adolescents and adults. If these individuals are endowed with a positive developmental potential then stress and frustration serve for them as basic developmental stimuli.
9. Specific Crises at Successive Stages of Development
Erik Erikson, (1950, 1959) in his contribution to Ego-psychology, has described specific conflicts characteristic for various stages of human development. He distinguishes eight stages of psychosocial development, indicating specific nuclear conflicts for each stage. These eight stages and eight kinds of crises are as follows:
1) Trust versus Basic Mistrust
2) Autonomy versus Shame and Doubt
3) Initiative versus Guilt
4) Industry versus Inferiority
5) Identity versus Role Diffusion
6) Intimacy versus Isolation
7) Generativity versus Stagnation
8) Ego-integrity versus Despair
According to Erikson (1950) human development proceeds through overcoming characteristic crises at each successive stage. A proper solution of a given crisis depends on the success in dealing with the previous one. Erikson’s concept of synthesis and resynthesis in the development of personal identity suggests a similarity with the concepts of positive disintegration and secondary integration of development. This similarity, however, is only apparent, because in our conception of develop-
244
ment the chances of developmental crises and their positive or negative outcomes depend on the character of the developmental potential, on the character of social influence, and on the activity (if present) of the third factor (autonomous dynamisms of self-directed development). One also has to keep in mind that a developmental solution to a crisis means not a reintegration but an integration at a higher level of functioning.
Although Erikson’s theory of crises is a very interesting attempt to characterize the various stages of man’s development, this position is based exclusively on psychoanalytic dynamisms without sufficient recognition of the influence of heredity, of various experiences in life together with influence from others, and especially of autonomous factors in development.
Moreover, Ego-psychology does not sufficiently underline the phenomenon of levels in the development of specific functions or groups of functions. Erikson’s views represent a rather mechanistic approach to the opposing relations between the dominant tendencies of each stage. Our viewpoint is that many of these paired characteristics are not in opposition but rather in mutual collaboration in development, for example, trust and mistrust, autonomy and shame, initiative and guilt, industry and inferiority, etc., because as generators of multilevel conflicts they build the inner psychic milieu and advance the progress of multilevel disintegration.
I believe that the recognition of the phenomenon of levels in evolution of the inner psychic milieu is necessary before one can attempt to understand the very complex dynamics of stages and crises in the development of man.
The theory of positive disintegration is not concerned with specific conflicts at various developmental stages. Both theories stress the importance of critical periods in achieving a new integration. Our theory does not recognize as many stages or critical periods as are claimed by Erikson other than the developmental periods recognized by the majority of psychologists. Crises, in our view, are brought about through thousands of different internal and external conflicts, resulting from collisions of the developing personality with negative elements of the inner and external milieus.
245
10. Lindemann: The Role of Crises in Personality Development
Among the theories which emphasize the importance of crises in personality development, the “theory of crisis” of Erich Lindemann (Lindemann and Klein, 1961), brings up the element of the so-called emotional hazard: a disturbance of homeostatic emotional equilibrium. Examples of such crises are provided by the loss of significant emotional attachments, involvement in a new social orbit, beginning of adolescence, marriage, achievement of professional standing. Etc. A crisis is reflected in an acute disturbance which may take place as a result of an emotional hazard. Attempts at solution of such conflicts may result in the recovery of the former emotional equilibrium, or in the formation of a more healthy condition of integration. However, if the problem encountered is of a level above that with which he can cope, an individual may regress to a lower level of integration. Lindemann emphasized the importance of one’s relations with so-called significant personalities. Significant personalities may well influence the solution of the crisis for the better or for worse.
By way of comparison, the theory of positive disintegration recognizes the importance of both the inner psychic milieu and of the external environment in the development of a crisis (Dąbrowski, 1967; Dąbrowski, Kawczak, and Piechowski, 1970). However, our main emphasis is on developmental tension and on those inner conflicts which are connected with the realization of hereditary endowment. Our theory views the external stimuli as acting on the tension (which will vary in degree and intensity in different individuals) of the developmental instinct, of creative tendencies, and of the tendencies for self-perfection through the process of positive disintegration.
11. Therapist-Client Relationship as a Condition of Growth
Carl R. Rogers (1951) developed the theory of a client-centered therapy, involving a specific relationship between the therapist and the client. Development of the therapist-client interaction determines the evolution of the psychotherapy and its outcome, and allows for a proper psychodiagnosis. The development of this relationship may also be fundamental to
246
personality development and thus play a role in therapy. Diagnosis becomes a result, as it were, of this therapist-client relationship.
Psychotherapy based on the theory of positive disintegration is closely related to this kind of therapist-patient relationship. However, in recognizing the possibility of a final diagnosis resulting from this relationship, we maintain that, prior to this final diagnosis, a universal diagnosis in its psychiatric-psychological and social aspects may be necessary as a basis for planning a psychotherapeutic program (see Ch. 13, Section 1)
One point of difference between Rogers' theory and the theory of positive disintegration is that Rogers gives environmental factors a predominant role, whereas we postulate a three factorial determination of personality development (developmental potential, external environment and autonomous factors). We are in agreement with Rogers (1964) that the basis for the hierarchization of discovered values is in the organism and among others, in the history of a psychoneurotic and his crises. Another difference is that Rogers' approach is to wait for the client to take the initiative. Yet in our view, in the case of special types of patients, there is a need for a quick initiative on the part of the therapist when clinical intuition indicates that the patient needs an immediate realization of a program of help.
12. Psychoneurosis as a Failure of Self-Actualization
In Maslow’s view (1962), neurotic symptoms, conflicts, feelings of guilt, anxiety states, depression, frustration, psychological tension, shame, self-punishment and inferiority feelings all create pains and troublesome complications in the efficiency of work. The symptoms cannot be controlled. The neuroses and psychoneuroses, generally speaking, are held to constitute a state of diminished development. They are not considered by Maslow to be altogether inconsistent with the development of mental health, but nevertheless, of development in such a direction that is devious and of a weak tempo. To some degree, the neurotic conditions are viewed as expressive of failure in personal growth. Maslow seems to interpret the psychoneuroses as representing a weakness in the capacity of a person for
247
the healthy realization of self, as a diminution in humanness. Neurotic individuals realize their humanness in inappropriate ways, the weakness in their development being based on the weakness or even loss of the system of values. Behavior is disintegrative and disassociated. Hence the effects of behavior will be more or less disorganized, and inappropriate to the effort expended.
In brief, Maslow differentiates healthy adaptation from unhealthy adaptation, healthy guilt feelings from neurotic guilt feelings, and healthy experience with psychic pain from the neurotic experience.
But let us take caution in interpreting Maslow’s position with regard to the psychoneuroses. First, it may be observed that where the experience and processes of psychoneurotic people are being considered, a specialist’s interpretation may take either of two directions, He may propose that psychoneurotic processes, in broad prospect, comprise integral elements of accelerated development. Or, even if he recognizes the rich existential contents of psychic life, he may declare that psycho-neurotic processes are pathological in their composition and direction. It seems to me that Maslow is closer to the second of these positions. Psychoneurotic symptoms are conceived in negative terms as being marginal to normal development.
Nevertheless, with the adoption of sound psychotherapeutic methods, Maslow would appear to consider that the psychoneurotic may be brought towards self-actualization. Not only this, but he would be among those who see in the psychoneurotic person, in addition to certain pathological dynamisms, some dynamisms which are creative. Emerging from their tragic and conflicting dynamisms are even some therapeutic and self-directing processes of a positive, developmental significance. Maslow allows that the growth of healthy self-realization is promoted through various grades of intellectual and emotional life. His view of the neuroses certainly reaches beyond the traditional medical-psychiatric model in that he sees in them a forward movement toward health and the realization of human needs. But at the same time, this forward movement is characterized by special attributes of anxiety and disquietude
248
which are interpreted in a pathological sense rather than as representative of courage and clarity of developmental direction.
My own observations have led me to note that symptoms of nervousness and the like, characteristic of the psychoneurotic, are also to be found in the so-called psychically normal person (i.e. those with a capacity for development), or in those who distinctly manifest aspiration towards mental health. To put it another way, the very same symptoms may be designated as either neurotic or healthy. The decision as to which categorization properly applies will depend upon the kind of psychological tension or disintegration, on the effects of the symptoms, and perhaps on some relatively obvious features of the symptoms such as creativity and tendencies towards autopsychotherapy. Just the same is true insofar as adjustment and maladjustment are concerned. It is necessary to differentiate between adjustment and maladjustment in terms of the conditions which have given rise to a particular psychic state. Perhaps in the developmental perspective my own views have something in common with Maslow’s, particularly as regards the fact that some psychoneurotic developments are subject to “negative regression” while the majority follows positive evolution through an “individual drama of personality growth.” Both Maslow and I underline that the course of development depends on the strength and character of the developmental potential, on the strength and character of environmental influence, and on the strength and range of activity of the third factor which stands for the autonomous dynamisms of self-determination.
13. Psychoneurosis as a Consequence of Guilt
Mowrer (1961) conceives the essential origin of psychic difficulties, or psychoneurosis, in autonomous factors. He rejects; genetic and environmental explanations of etiology in favor of the view that each individual is responsible for his own life and further, for his own sickness. Illness, then, is the effect of a person violating his own system of values and his own consciousness. Hence are derived guilt feelings which do not constitute a sickness. Rather, they are a consequence of a person’s lack of responsibility in the practice of inappropriate and amoral behavior.
249
The most frequent reaction to the foolish or even bad things one has done is to deny their existence. But for those with any measure of sensitivity, the “hidden” guilt may present considerable psychic tension and difficulties of different degrees of strength. These symptoms of illness Mowrer has described as the amplified and distorted voice of conscience. They are effects of the expression of conscience which act from something which is hidden, and speak, as it were, through our body, our emotional life, and our behavior.
The tendency to enclose all of one’s bad acts within oneself draws a person away from the social group. The contrary, the tendency to be open, brings him back towards participation in social life. It also contributes towards authenticity in living. Openness alone, however, is not held to be sufficient to lift the feelings of guilt and their pathological effects. Also necessary is both the affirmation of one’s own failure and the compensation of these who have been in some way wronged.
Mowrer’s “integrity therapy” calls for confession as a condition of return to moral, psychic integration. Confession cannot be superficial, invoked, perhaps, to justify guilt in terms of prevailing conditions, but must incorporate a deep analysis of one’s own faults, lacks and transgression of moral law. Psychotherapy should take some initiative, and takes, place best in a group where the individual may subject himself to the opinion and judgment of others. This approach strongly emphasizes the importance of a person’s own effort and actions which are held to be a necessary component of confession and part of the first stage of therapy.
Restitution for wrong conduct, then, is a central element in therapy. The rationale here is the release of positive feeling as a consequence of appropriate action.
In comment upon this theory, four points may be raised. The system has particular strength in recognizing the place of autonomous and moral factors, the hierarchy of values, responsibility and the “open group” as contributing to the processes of autopsychotherapy. Second, Mowrer offers a useful insight into the dynamics of positive development by stressing the place of guilt feelings in the genesis of psychoneurosis and by
250
stressing the need for reparation (taking on responsibility) in therapy. Third, I cannot wholly accept Mowrer’s view of the dynamics of guilt feelings, i.e. whenever there is the feeling of guilt there must have been a transgression, on the grounds that many eminent people who have advanced in self-perfection, still present strong guilt feelings. A more appropriate interpretation of such feelings as far as I have derived from most of my cases, might be to see them as an expression of the distance between a person’s ideal and his own view of his inner reality. Understood in these terms, guilt feelings may be seen to play a developmental role as the perception of a distance from one’s: personality ideal, and perhaps, as the perception of transgress-ion against this personality ideal, which, after all, we postulate to be the highest dynamism in the development of personality. Lastly, it may be suggested that group therapy, and confession in the presence of a group, are not always indicated as unique and even necessary components of treatment. There are many who, because of their particular psychological type, or even because of their own life-history, cannot become participants in group therapy and cannot engage in unrestricted exteriorization among people whom they barely know.
251
CHAPTER XIII
PSYCHOTHERAPY OF PSYCHONEUROSES
1. Principles
In this chapter we shall discuss briefly the principles and methods of psychotherapy in psychasthenia, psychoneurotic obsession, psychoneurotic depression, psychoneurotic anxiety, and psychoneurotic infantilism. The general principal which is of fundamental importance for diagnosis and subsequent psychotherapy is to find out whether a given psychoneurotic process is a part of a unilevel or a multilevel disintegration. During psychotherapy we have to keep that in mind and adapt therapeutic techniques accordingly.
A universal diagnosis embracing the psychiatric, psychological, and social aspects is a necessary basis for planning the program of psychotherapy.
This basic diagnosis we call a descriptive-interpretative diagnosis in order to distinguish it from a clinical diagnosis which categorizes individual cases according to a classification of syndromes.
The descriptive-interpretative diagnosis is a multidimensional and multilevel approach which includes the assessment of neurological, psychiatric and social factors in the life of the individual. This diagnosis is based on a developmental point of view in relation to the so-called mental disorders. It takes into account the richness, originality and the creative elements of “pathological” processes following the assumption supported by clinical experience and systematic investigation that the conflicts of life, nervousness, and psychoneuroses are in positive correlation with creative abilities. The aim of the diagnosis is to grasp all the positive factors, to introduce the patient to them and to make him a co-author of his diagnosis. In this way the diagnosis
252
constitutes an integral part of therapy by introducing the patient to an experiential discovery of the creative elements of his “disorder.”
The multidimensional, detailed and synthetic diagnosis comprises essentially half of psychotherapy; it is especially valuable in cases of patients with multilevel development. For most patients the discovery of their originality, creativity, symptoms of accelerated development and even talents, and the program of development of such functions, very often gives them a clear sense of life.
(1) Psychasthenia
In the psychotherapy of psychasthenia we are concerned with the stimulation at a higher level: the stimulation and development of creative forces, increase of prospective tendencies, awakening or increasing the patients faith in his own powers and his own worth. From time to time one has to work on improving his reality function at the lower level in order to counteract the tendency for separation of the higher and lower levels of functioning with consequent neglect of the practical aspect of living.
(2) Psychoneurotic obsession
In psychotherapy of psychoneurotic obsessions, or of obsessional factors in psychasthenia, we have to endeavor to increase the interests and creative capacities of the patient, to separate his obsession and the activities of his daily life into, two channels, so that the latter may be exercised with a certain feeling of responsibility, in spite of the obsession. We should go as far as to introduce into the patient’s daily life certain obsessive elements which may have a positive develop-mental effect, such that the totality of obsessions (first channel) is reduced while the “positive” obsession introduced into, daily life (second channel) loses its pathological influence.
It is important to introduce elements of joy and satisfaction into the patient’s life by reinforcement of his creative tendencies, by convincing him of their value. It is also important to improve his position in the family as well as in society, for very often such psychoneurotics are treated worse than other
253
members of the family; very often they are compared to others, presumably more successful, and told to imitate them, which is nothing else but a humiliating way of telling them how inferior they are. It is thus necessary to make the other members of the family aware that such attitude is inappropriate, if not harmful, and to show them the attributes and values (often hidden) of the psychoneurotic. In this way his position in the family, and thereby in the society, may be improved.
Finally, it is necessary to raise the level of the obsession to a higher plane, reinforce its developmental character and its positive coupling with daily life, in order to organize in its structure new forces in the service of personality. This can be accomplished by showing convincingly enough to the family and to the psychoneurotic the positive and creative aspects of his obsession, such as for instance his excessive anxiousness over his family, or his feeling of the exclusivity of the bonds of love, etc.
An attempt at regulation of daily life, in its private and social aspects, has a decisive importance here for the loosening and disintegration of those negative elements which are the main factors in the growth of obsessional forces.
(3) Psychoneurotic depression
Concerning psychoneurotic depression basic psychotherapeutic indications are as follows: Making the patient aware of the positive possibilities of his depressional conditions in the sense of convincing him what creative role may be hidden behind his periods of alternating excitement and depression.
One has to show him that both phases of the depression-excitement cycle have creative elements. The phases of depression increase his feelings of inferiority, insignificance, humility, self-analysis, and self-criticism, while the phases of excitement enhance inspiration, vividness of associations, facility of synthesis, awakening of new ideas, etc. One has to demonstrate how the development of critical attitude to both these phases is of great advantage in development because it promotes the dynamic perspective of “subject-object in
254
oneself.” In this way one may lead the patient to a stronger understanding of the positive aspect of his states and at the same time reduce and minimize harmful pathological tendencies related to his states. These psychotherapeutic maneuvers will be much easier when the patient has already some dynamisms of spontaneous multilevel disintegration.
Behind the I of depression there may be hidden a developmentally necessary psychological withdrawal serving the function of self-criticism, self-analysis, self-control, a justified dissatisfaction with oneself and feelings of inferiority with respect to one’s own possibilities. If these processes can be found in a depression they indicate a potential for positive growth.
The development of self-control and inner psychic transformation can be effected through the binding of symptoms of depressive psychoneuroses with the entire process of multilevel disintegration and secondary integration, that is to say, participation of both controlled phases of depression in cooperation with the main dynamisms of development, such as: the third factor, disposing and directing center at a higher level, dynamization of personality ideal.
(4) Psychoneurotic anxiety
With respect to psychoneurotic anxiety, it is important, whenever applicable, to uncover the connection between the anxiety conditions of individual experience and those of a universal character, having a general existential nature and being characteristic of high moral development. It is important to bring the patient to the realization that some of his conditions of anxiety, decreased activity, fear, and a tendency for ekklisis (Monakow and Mourgue, 1928), usually indicate positive developmental possibilities. It is essential to link the “pathological dynamisms” with the most important dynamisms of secondary integration on the one hand, and on the other to provide means for the release of tension such as relaxation therapy, stimulation of interests and abilities, opening of new interests, improvement of family relations, etc.
255
(5) Psychoneurotic infantilism
In therapy of psychoneurotic infantilism it is necessary to assist in appropriate transition to positive regression; to help in organizing the development of creative abilities; to develop insight into some positive values of depressional conditions, and into other dynamisms of positive disintegration. This may be done by direct psychotherapy with adults, youth or even some children, as well as by indicating helpful literature such as biographies of outstanding people and by proper encouragement in becoming acquainted with it.
It is also very important to organize a warm and supportive milieu, especially in the case of children; to develop contact with nature and to organize a healthy energy release (sport, much time spent outdoors, in the country, etc.).
And, finally one works on the gradual development of control and strengthening of affects.
2. Individual Cases and Treatment Programs
Before giving the material of the cases we shall briefly outline characteristic types of enhanced psychic overexcitability, levels of disintegration, types of psychoneurotic processes and the kind of psychotherapy appropriate for each case. A fuller comparison and differentiation of individual psychotherapeutic programs is given at the end of the chapter. Table IV gives a summary overview of the diagnosis and therapy of the six cases.
The first case (S. Mo.) is characterized by enhanced emotional and intellectual overexcitability with some admixture of sensual and psychomotor (masturbation, obsessive need to arrange things in perfect order). Emotional overexcitability finds its expression in the states of anxiety, intellectual overexcitability in the obsessive questioning of the meaning of life. S. Mo. As an introvert tended to search for solutions to his problems in his inner psychic milieu. At this time his inner psychic milieu was too poorly developed to provide a clear path of development leading toward a solution. In consequence his tensions grew high, his obsessions had little chance of being channeled, his sensitivity and
256
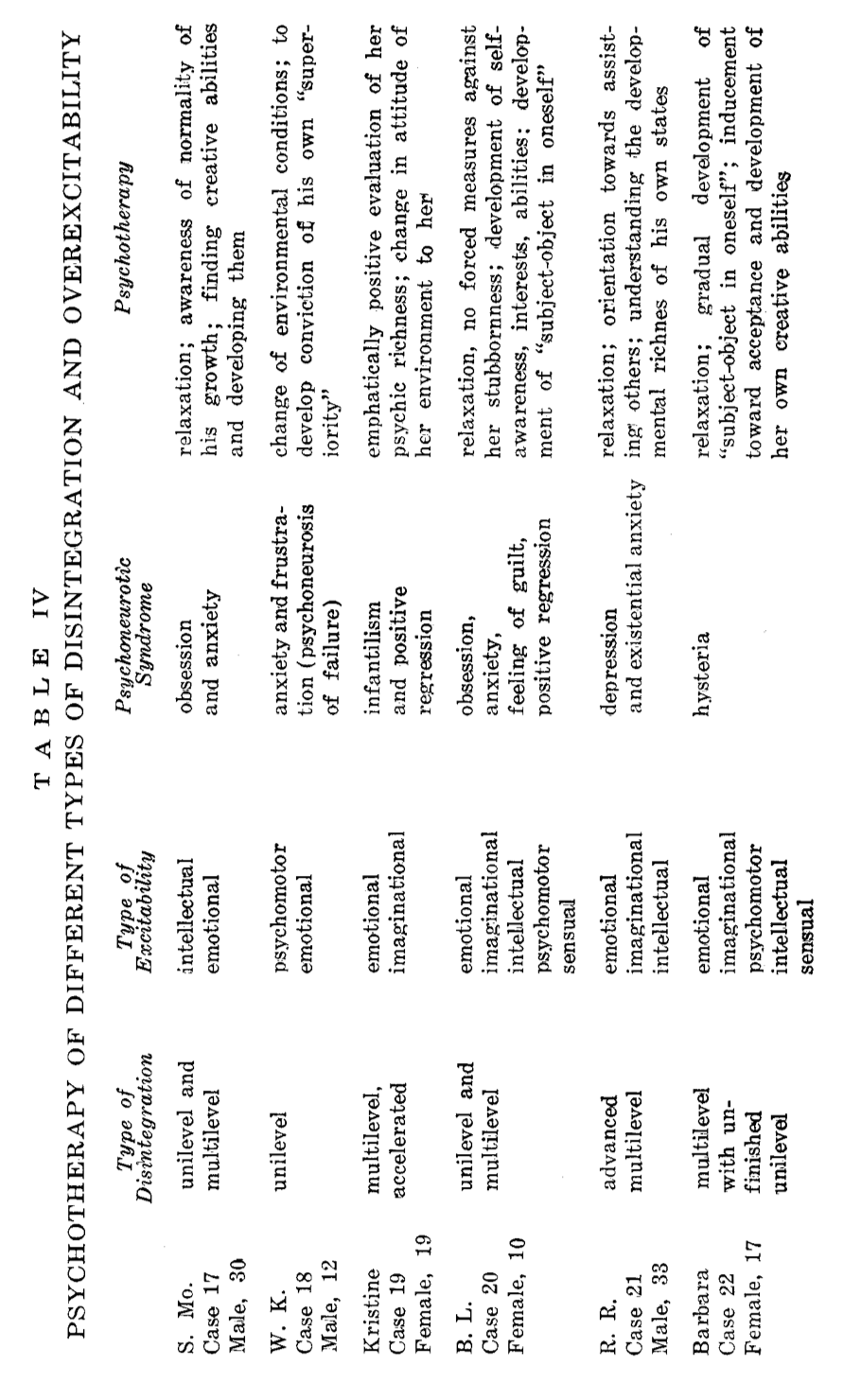
irritability to the external environment were amplified because of the conflict with his introverted nature and his strong feelings of emotional exclusivity.
The high tension of his anxieties and obsessions is related to the stage of mixed positive disintegration (unilevel-multilevel) which is the hardest to resolve. The solution is possible only through the growth of hierarchization of the inner psychic milieu, and at this borderline stage hierarchization is not very strong as yet.
Psychotherapy of S. Mo. Followed two main directions: one of relaxation and decrease of tension at the start of his work and thinking, the other of convincing the patient of his intellectual, moral and creative assets not only to reduce tension but to provide him with the conditions necessary to move to the stage of multilevel disintegration.
The boy W.K. (Case 18) manifests enhanced emotional and psychomotor excitability, the latter being expressed psychosomatically as bed wetting. He is predominantly an introvert with a strong feeling of inferiority (bed wetting). Negative self-concept, poor hierarchization and unfortunate accident further enhanced his immature introversion and sensitivity towards the external world. His stage of development can be described as unilevel with fairly well stabilized nuclei of multilevel disintegration. The whole picture, however, was of psychoneurosis of failure.
At this level of disintegration psychotherapeutic rescue can come only from the outside. The therapy of this boy went in the direction of giving him the convincing experience that his abilities were as good as anyone else’s in his family and in school, and that in some respects (creative technical abilities) he was even superior to others.
Kristine (Case 19) is characterized by emotional and imaginational overexcitability and an accelerated process of multilevel disintegration. The factors accounting for her advanced stage of development were positive traits of childishness, creative abilities, sensitivity and charm, and marked growth of self-awareness and empathy. In her mental structure Kristine had strong elements of developmental defense, one of them
258
being the gradual formation of a disposing and directing center at a higher level. The main “pathogenic” element of her case was an inappropriate evaluation by her family. We could diagnose her case as psychoneurotic infantilism, which in itself contains prophylactic and developmental elements.
The essential direction of Kristine’s therapy was to promote her creative awareness and consolidation of her inner psychic milieu and to reduce the negative influence of her environment.
The ten-year-old girl, B.L. (Case 20) represents a combination of all five forms of psychic overexcitability. The strongest are emotional and imaginational components. This multiple mixed character of her overexcitability represents strong developmental potential, nevertheless, it is also a cause of excessive psychic tension. Her developmental stage is a “balance” of unilevel and multilevel disintegration. Her chief “pathological” symptoms were excessive excitability and obsessiveness, combined with easily evoked scruples and feelings of guilt, and excessive tensions. By her “positive regression” to behavior of earlier childhood she showed tendency to autopsychotherapy (relaxation, diminution of difficulties).
Her psychotherapy called for prevention and reduction of her tensions in order to make possible the growth of her originality and psychic richness, which by themselves are strong prophylactic and developmental factors, and therefore therapeutic. In her case one may also start to slowly awaken the nuclei of her dynamism “subject-object in oneself.”
In the case of R.R. (Case 21) we encounter the very important mixture of emotional, imaginational and intellectual overexcitability. These combined forms of overexcitability bring about an enhanced intellectual penetration which expands perception of reality. In turn this expansion serves the further development of these components of the developmental potential. R.R. saw and experienced the tragic aspect of existence, its cruel and unjust stresses; he felt an altruistic “pain of existence.” His disintegration has reached advanced level III with great potential for further development. As for diagnosis R. R.’s condition can be described as psychoneurotic anxiety of the existential type with strong depressive components.
259
R. R.’s psychotherapy was directed towards developing his understanding that from the point of view of mental development he was healthy, that he was endowed with rich inner psychic milieu. This richness can be seen in the high level of his empathy, his dynamism “subject-object in oneself,” and his hierarchical conflicts. It was necessary and not too hard for R.R. to understand that he had to pass through these states and levels in order to be able to better understand the difficulties and existential crises of others. By his psychic richness R.R., appears designated to understand others and to help them and this entails a high level of responsibility for others.
Barbara’s case (Case 22) is an example of the combination of all the forms of overexcitability although in different constellation of intensity. Imaginational and emotional components are predominant showing the greatest tension. This constitutes her great richness and at the same time great strength. At the time of the interview she was undergoing a rebellion, quite understandable and justified in view of the breakdown of her family. Her aggressiveness was not tempered by higher levels of an inner psychic milieu still insufficiently developed in her. In consequence she made sweeping negative generalizations about all the members of the human race.
Diagnostically Barbara represents a hysterical constellation at a fairly high level with elements of depression, aggressiveness, and even obsession.
In psychotherapy it is necessary to lead her to a deeper self-awareness, to help her overcome the one-sidedness of her judgments, to develop in her some understanding of different levels of development, and to gradually help her develop come degree of humility.
(1) Case 17
S. Mo. Was a man 30 years old with tetanoidal traits (according to Jaensch, 1923), i.e. with a tendency to muscular twitching, spasms, as in tetany. He was also inclined to depression, anxiety, and avoidance (ekklisis). He was obsessed with perfectionism and the need for order. He had irrational fears of an imminent misfortune; at times it took the form of neurotic
260
inability to start work, to reach a decision. This “neurosis of procrastination” can sometimes be observed in high school students who prepare everything for their homework and then sit for a long time incapable to force themselves to start.
S. Mo. Was a person of considerable emotional sensitivity, of excessive tendencies to emotional exclusivity, and of great responsibility for his work. He had definite tendencies for evaluation of reality in forming a hierarchy of values.
There were no definite traces of childhood frustration. The patient was given to rather strong masturbation at puberty, and periodically later on. Here is a transcript of the third session with this patient.
K.D.: Are you very much impatient when you find your desk in disorder and other things out of their usual place in your office?
S. Mo.: Yes, this irritates me very much.
K.D.: Has this need for excessive order persisted since childhood?
S. Mo.: Yes, from early school days, but the symptoms were less strong at that time.
K.D.: Are these little disorders really so important—and what exactly irritates you in particular?
S. Mo.: It is usually because I come in with strong psychic tension, under the influence of unpleasant contacts with people, but also the fact that I have some interesting thoughts “in my head” which I would like to work through, and then precisely I must pay attention to ordering the room and prepare everything for writing. This disturbs the content and the order of my thinking.
K.D.: That is entirely understandable. You are creative, and your thoughts make you tense, is that right?
S. Mo.: I would think so.
K.D.: It is necessary for you to express these thoughts. On the other hand, I realize that your thoughts and experiences often concern things of great importance, which is appropriate and extremely significant. You were telling me at one time, that you are aiming at perfection. Would you not think it
261
advisable to concentrate there still more, to bring there your dominant attention, and then be ready to start the work immediately without putting the room to order. Would it not be good—and I would like to have your definite opinion—to put things in general order on the desk within a minute or two, relax for a moment—and then think or write?
S. Mo.: Probably so, Doctor, yes, it would be good.
K.D.: Last time we were just talking extensively about the autogenic method of relaxing. Would it not be good, if you would, after coming home, and making this little bit of order we mentioned a minute or two ago, relax and then think about these important things which occupy you so much?
S. Mo.: I started to do it already after we talked about it the first time.
K.D.: You were telling me that you often have disquietudes, anxiety conditions, at times even dread. As we were discussing it already, therein are hidden strong creative elements and it is necessary to help them in their proper development. The fact that you do not practice enough relaxation leaves too much tension and at times reduces your creative elements. We talked already that your conditions of anxiety connected with strong tension are understandable. It seems to me that you have a considerable endowment for the development of the sense of responsibility for your family and for society. There is not only the endowment; the realization of this responsibility is already being developed as well. Something, however, is not quite harmonized here, and it seems to me that you do not balance your excessive tensions and anxieties with the attitude: “I am doing all I can and will try to do more. In trying to have always a human attitude of understanding, helpfulness, avoiding wrong, but with whole-hearted cooperation, I should be able to go on that road with increased understanding and feeling that nothing can detract me from what I am doing.”
S. Mo.: Yes, that is very right and I was behaving like that often, but at times I have such periods of doubt, such conditions of fear of the unknown, that I can hardly keep a hold on myself.
K.D.: This might diminish, after putting to practice all that
262
which we were talking about, but in some of these cases you cannot keep fighting or eliminating them from yourself since this would make you morally and psychically impoverished.
Now let us go on from here. Fortunately or not, your emotional exclusivity, your sensitivity of emotions must be connected with anxiety. It is difficult to talk here of curing, for this should not be cured. These feelings may only be balanced through their more intimate connection with greater understanding of your condition and your acceptance of responsibility for yourself and for many things of a social nature. I know that your writing tends in that direction; but this should be further strengthened. Perhaps you will not be amazed that, rather than decreasing your sense of responsibility, we are trying to build it up. But this is the right way in your case, I am sure.
S. Mo.: I understand this well enough, and I have no doubt that in my case this is the proper way. However, with all my doubts, I am glad to have a confirmation on your part.
K.D.: We both know that a fundamental trait of your personality is evaluation of reality, and, therefore, in your case also evaluation with respect to yourself. I hope you will pardon me if I say a few words about it; pardon me, I say, because I know that you think about it and you may perhaps understand these things more than I do. But—you see—I believe that someone’s objective and friendly thoughts may confirm and strengthen one’s own attitude, and you do not doubt what my attitude is toward you. There is, you know, at times a certain amount of lenience necessary for oneself in order to extend it with understanding and indulgence towards others. You feel very much that your evaluations are connected with excessive psychic tensions. You were once telling me of such tension in your assessment of others. Perhaps it is advisable to foster more lenience for both yourself, and others, before you can achieve a status where a greater kindness toward others may accompany greater severity towards yourself.
And now, concerning other things to do—you know them well enough. Much theatre, music, exhibitions, painting, and sculpture; quietude and contact with nature, systematic recourse to relaxation, smiling and laughing, and some gymnastic and sports.
263
Interpretation of psychotherapy, on the basis of the theory of positive disintegration.
S. Mo. Was an individual of high emotional and psychomotor excitability (he had a great need of doing something); he was introverted and had a strong tendency for emotional exclusivity (his feelings for his family and friends were very deep but limited to a few individuals; he had a major interest in human individuality). He represents a strong feeling of responsibility related to hierarchization. His slight tendency for obsession, only initial phase of inner psychic transformation had, however, some preponderance of unilevel over multilevel disintegration. His punctiliousness and small obsessions had a unilevel character. He had not yet awakened in himself the forces moving towards secondary integration, because his dynamisms such as “subject-object in oneself,” the third factor, and personality ideal were still too weak. Since he has not yet come to introduce some organization into his course of development this was the basis of his difficulties in the formation of a disposing and directing center at a higher level and in the dynamization of his personality ideal. In other words he was still far removed from attaining the stage of organized multilevel disintegration. These weaknesses did not provide an adequate basis for hierarchization at a higher level, nor did they allow him to realize such a hierarchization. Hence, his hypersensitivity to external conditions and consequent appearance of certain anxiety states and excessive tension. This, of course, is related to the fact that his unilevel processes were still strong and created excessive tension in his higher, multilevel dynamisms (e.g. feeling of responsibility, exclusivity of emotional bonds).
In psychotherapy—as we saw from the interview, we were concerned first of all with decreasing the patient’s inner tension, his tendency to scrupulosity, in order to reduce his excessive feelings of responsibility and achieve a greater measure of psychic harmonization with ensuing control of himself and his own external environment.
Psychotherapy was then conducted such as to promote his sense of personal dignity, to convince him that his most important tendencies are based on a very positive structure,
264
that they are psychically valuable, and are indicative of a possible accelerated psychic development.
To this end, during various sessions, the positive meaning of certain symptoms of disintegration was emphasized. Such action by decreasing his tensions reduced an improper relation of the patient towards himself. The treatment tended to reduce “obsessive attachments” and improper defensive forms such as, for example, a compulsive need for order.
Our attitude was also positive towards the patient’s creative abilities; we attempted to increase them and to form—together with the dynamisms of multilevel disintegration—a stronger nucleus of a disposing and directing center at a high level.
As we saw, a method of relaxation was also recommended, derived from Schultz’s method (Schultz and Luthe, 1959) as well as contacts with different forms of art, with nature, and solitude.
(2) Case 18.
W.K. was a 12-year-old boy who had gone through a rather serious scarlet fever while about 6, without, however, any detectable organic damage. After this sickness he started to exhibit symptoms of fatigue and considerable emotional sensitivity. He slept badly and woke up often at night.
From the time of early childhood, he showed emotional and psychomotor excitability, with involuntary bed wetting since the age of 3. There were no other disorders.
When he started school, he developed a fear of reading, and often while answering in class he would suddenly grow weak. Some of his poor school grades he took with great difficulty. In addition, a finger of his right hand had been injured (the terminal digit was cut off). His excitability was increasing, he began to show anxiety of an obsessive type; he was jealous of his brother and sister who were neither so excessively sensitive nor cried so much over their failures.
The boy, because of the above factors and excessive yielding to the flow of involuntary associations (a sign of strong emotional excitability, tension, preoccupation with difficult
265
problems), fatigue, had difficulty in concentrating his attention and began to be noted as a poor student, which in turn increased his feelings of inferiority.
His typological traits (emotional and psychomotor excitability, irritability, moodiness, some introversion) did not facilitate his contact with his schoolmates; this caused an increase of his tendencies for isolation and created new problems which further augmented his inferiority complex. In this way a “vicious circle” was formed.
The boy exhibited even stronger than before anxiety states, of inhibition and “pathological rumination,” which were compensated through an increase of emotional and psychomotor excitability (tic-like movements), and eventually led people to be concerned about him, and even more so to his drawing excessive amount of attention to himself.
His psychic tension was high, so that he came to believe that he was a failure. He felt inferior to other students and to his family, he thought himself worthless and felt rejected. In consequence his tensions and anxieties grew, and so did his inclination for isolation. He did like school. He also liked fixing children’s toys, little cars, etc. Often he had creative technical ideas for new mechanical toys or how to improve them. He liked to be left alone in his room to be occupied with do-it-yourself toys, or drawing.
Usually he had no dreams, at times however “strange beings” came out in nightmares and chased him; then he would hide in his father’s or in his own room.
His father was a quiet, well balanced man, and quite concerned for the boy. His mother exhibited excessive emotional activity, at times explosive, and voiced in an improper way the difficulties she had with her son in comparison to other children; she did this often in the boy’s presence. His sister was a few years his elder, but was away from home. A brother, younger by four years, presented no educational difficulties. The home atmosphere was generally fair, the parents did care for their children, although the mother was not always right in her decisions, and, unfortunately, rather sure of herself.
266
The boy was treated in a psychiatric ward. He went through a detailed examination, and was treated with a variety of drugs. Diagnosis was of post-scarlet fever encephalopathy, with EKG unchanged.
Neurological examination:
Excessive muscular and abdominal reflexes, testicular reflex somewhat wide, red dermographia strong and of long duration. Chwostek reflex positive on both sides.
These responses indicate enhanced psychomotor and emotional excitability. In anxiety states and at this stage of development increased abdominal and testicular reflexes are frequent. Strong and extended red dermographia points to a functional disturbance of the neurovascular system. Positive Chwostek indicates a reduced level of blood calcium, and psychologically “spasticity.”
Psychiatric examination:
Increased emotional and psychomotor excitability, tic-like symptoms (i.e. tics not clearly developed) occasional tics.
Psychological examination:
Normal intelligence, Rorschach and TAT give a picture of anxiety, weak social contact, tendency to isolation and strong psychic tension. Capacity for inner psychic transformation appears not too strong. Definite symptoms of depression.
Interpretation:
The boy has increased emotional and psychomotor excitability, with an excess of introvertive traits, a definite history of failure in family relations and especially at school, a so-called “jinx” quality, and is a victim of stereotype psychiatric and educational classification.
With introvertization, inhibition and anxiety states related to a lack of his own place in family and school reality—he arrived at a wrong evaluation of himself.
267
His rather pronounced suggestibility and autosuggestibility with regard to external and internal stimuli operated on a low level. It means he was lost in concrete reality by accepting the suggestions and influences of his environment without doubt or criticism; he thus failed to make himself aware of the worth of his own abilities and his own moral judgment.
His attempts at “taking care of himself” have resulted in psychoneurosis of failure” with excessive emotional instability, feelings of helplessness with regard to any attempt, feelings of failure and of being lost, with several forms of negative compensation such as strong psychoneurotic tension, tic-like movements, isolation, etc.
Psychotherapeutic indications;
Very careful selection of a good tutor, who, under specific psychiatric direction would conduct the entire educational program of the child, in contact with the school, and who—after some acquaintance with psychiatric examination and treatment, and directives regarding the boy’s abilities and his failures—would conduct a complete re-education. This would consist principally in strengthening the boy’s personal feelings of security, faith in himself, conviction of personal talents, explaining causes of failures within a scheme of a well-guided; detailed program.
Leading the boy to participation in skating, skiing, swimming and achievement of some standing in one or another of these, sports would be very helpful. It is also advisable to introduce the boy to special rhythmic exercises involving the whole body. These exercises called Rhythmoplastic are designed to develop the psychophysical coordination of the expression of the movements of the body.
Under these conditions attempts should be made to have the boy establish contact with a small peer group. It would be advisable that the boy help one of them in the development of technical abilities and repairs in which he is good. He should be helped in checking the results of his work in relation to such an “apprentice.”
It would be necessary to increase the mother’s sense of care
268
in relation to her son in general, and especially as regards her expression of negative opinion about him. Attempts should be made toward attainment of such conditions of a family atmosphere that the boy’s abilities would be recognized in some areas to be at par with those of others, and even in certain respects, superior to that of other family members.
Through occasional well prepared talks with his father or psychiatrist, the boy may be led to increasing self-control, without being depressed by momentary failure or overwhelmed by emotional reactions.
Psychotherapeutic elements based on the theory of positive disintegration would consist, first of all, in changing family and school attitude toward the boy, and of the boy’s attitude toward himself; in destruction of the present disposing and directing center at a low level, consisting of his crippling beliefs about lack of ability, lack of intelligence, contrary to what he was capable of. This boy was thus far governed by his anxiety, feeling of inferiority to others, dislike of his milieu, and isolation (avoidance)
The task of therapy would be to help to build a structure more solid than the unsteady ground of failure, anxiety, isolation tendencies and an inferiority complex but instead to promote the boy’s own self-respect, enabling him to find positive tendencies among his so-called psychopathological symptoms. It is important, too, to help in establishing the boy’s independence in his inner milieu to free him from the prejudiced opinions of his environment. In this way the power of suggestion of negative, and in this case harmful, criticism would be reduced and counteracted by suggestion of his positive qualities. This would be effective to the degree that the boy could generate these positive suggestions within himself. This would diminish his dependence on his environment but increase his independence and positive self-evaluation. This would amount to raising his disposing and directing center—such as one can, speak of—to a higher level.
Results: after some nine months of work—very considerable improvement. His passivity diminished, he was seeking isolation less often, while his self-confidence was slowly on the rise.
269
(3) Case 19
Kristine, a 19-year-old female student was delicate, subtle, creative, with a child’s smile, occasionally excessively spontaneous or direct, capricious, with strong excitability of imagination and affect.
She was considered emotionally underdeveloped, while intellectually well endowed; she was treated as emotionally immature and unstable. Though very good looking and a good dancer she did not care for boys. She was repulsed by physical contacts, even by the most subtle sexual advances from boys.
She liked dolls, fairy-tales and legends and had many-sided superior abilities, especially in art. She began menstruating at the age of 16; her menstruation was normal. She was treated by a gynecologist and an endocrinologist; no disturbances were noted. This treatment was rather shocking to her, she began to have outbursts of crying and sleeplessness. Light depression condition followed with a tendency for isolation.
Here is a transcript of the third session with her.
Kristine: Sir, would you tell me the truth, am I normal or mentally ill; I am scared of mental illness.
K. D.: Why do you insist, why do you specifically mention truth, Miss Kristine? You were telling me before that you do have confidence in me, could I possibly mislead you? Kristine: No, I am sure not, but lately I have many fears and anxieties and begin to lose confidence in people.
K. D.: I understand, my child—and I am sorry I used this word “child.” No indeed, not only are you not now nor are ever likely to be mentally ill, but, on the contrary you could be of much assistance to those mentally disturbed and—since you are in your first year of medical studies, I would certainly have made an objection as to your choice of profession. No, you have something in your very behavior, your attitude, your smile, something which indicates confidence, evokes joy, and really reassures and gives an optimistic outlook. Furthermore you have a need for helping people and you know how to direct them, if only some special circumstances do not cause anxiety and depression.
270
Kristine: You will pardon me, doctor, but you are wrong; I am not in medicine, I am studying to be a psychologist and that is not quite the same.
K. D,: I am sorry indeed, but somehow your looks, face and your whole attitude reminds me of a medical student. Yes, yes, now I remember—you are a psychologist and later on you want to add medical studies. I will be so glad to be of any help I can. I might be a little afraid because of your excessive sensitivity, but I have no objections.
Kristine: But so many people, especially my family tell me that I am not serious, that I am emotionally immature, hysterical, that “such fools are often quite capable, but nevertheless they are fools.” They often tell me that I am unrealistic, because I still like dolls and stories—and that this is impossible at my age.
K.D.: My dear young lady, please do not be disturbed one bit about it, but rather be content and desirous to retain this childlike attitude for quite some time; it may be very creative. Let me tell you that you are already someone quite outstanding and have a bright prognosis, that you will give much joy and of high quality to people and they will be proud of you.
This magic and fairyland thinking of yours, all this world of fantasy and theatre, is still more important in the influence on your behaviour, your spontaneity, sincerity and the definite sympathy you have for children. It indicates that you have considerable developmental tension and talents; your growth will be very long and intense.
Kristine: I am so glad to hear what you are saying, doctor, but why is it that others have so different a view of me? If you will pardon me, I have an impression that you are just trying to console me to strengthen me and make my life more easy.
K. D.: You are wrong, Miss Kristine. I always feel bad about consoling, pedagogizing or moralizing. But you see, I believe this is true. And if a doctor is not thinking about consolation in the first place. Let us accept such consolation. Because that is something entirely different from that which we usually attribute to the term “consolation.” Certainly such a definition
271
may have a therapeutic effect, but that is because it is endowed with what we call, as physicians, multidimensional consideration, that is to say, the capacity to view the issues from many sides and many levels. In literary terms this may be called “whence we came and whither we are tending,” and in psychological language “developmental dynamics” with recognition of past and future prognosis, that is with respect to both retrospective and prospective methods.
Kristine: Thank you, doctor, but I would like to put another question, of which I am simply ashamed—do tell me please, am I really underdeveloped psychophysically, or rather physically and emotionally because I had late periods, for which I have been examined by other physicians?
K. D.: It is not easy to say what is the cause of what. You know the term “psychosomatic.” In your case, the psychic side is stronger than the physical, even though the latter is quite in order. Simply, you brought into the world such psychophysical endowment, that you must have much more time for a deep, creative development and that is why you will be growing for a long time. This is a very common phenomenon among creative people. Simply, they have such a great developmental potential, “they have the stuff to develop” and that is why it takes them longer to give it full expression.
Interpretation of therapy from the point of view of the theory of positive disintegration.
From this brief description and dialogue, the patient presents a personality of fine intellect, of increased emotional excitability and vivid imagination, of considerable tendency for syntony and extraversion as well as introversion. All combined, it makes for strong developmental potential. She is creative, with a definite capacity for observation, self-observation and self-control.
Furthermore, she is susceptible to suggestion, and exhibits a tendency towards depression and states of anxiety. She is certainly psychically “fragile,” without showing however, any patterns of mental sickness.
272
The main dangers here are: susceptibility to the influence of the environment, to ridicule, weakness in character, considerable ease in accepting suggestion and autosuggestion.
In psychotherapy the aim was to strengthen self-confidence and objective observation of her own development, as well as an objective evaluation of her intellectual, moral and emotional abilities and attributes. This very strengthening of her awareness of her personal psychical security, based on objective evaluation of several positive attributes, permitted a slow reinforcement and growth of a “disposing and directing center” at a higher level. Since this patient was in a rather advanced stage of multilevel disintegration, with rather weak evidence of secondary integration, professional psychiatric help was very advisable in her personality development. It is important to help her to arrive at the stage of organized multilevel disintegration, to help in the development of more definite dynamisms of secondary integration, and provide assistance in development of a more mature view of herself. It is of basic importance, also, (and this was done) to arrange for a talk with a senior, more responsible and mature, member of her family in order to remove all elements of ridicule from the family atmosphere.
In this connection an attempt was made to explain what is meant by “emotional immaturity,” psychic infantilism and especially the continuation in her behavior of the so-called childish traits [cf. Chapter 5, Section 1(5) and 1(6)].
(4) Case 20
B.L. was a girl 10 years old.
She was highly excitable emotionally, sensually, and in the psychomotor and imagination areas. She was very capable, especially in the arts and humanities. She was attached to her parents, yet seemed fairly independent and stubborn.
Her parents were nervous, but controlled; the atmosphere at home was on high moral level. Besides B.L. there were two other children—a boy and a girl—all differently talented. There were occasional arguments and fights among the children due to typological and age differences. No traumas or repression
273
patterns of psychoanalytic type were noticed nor was there any discrimination towards the children on the part of parents. The girl was known from earliest childhood to have excessive excitability of imagination and emotions.
She lived in a world of fairy-tales, magic and animistic thinking, yet in spite of it she was a very good student. She loved her parents very much. She was ambitious and jealous of her parents' feelings but not pathologically. She was rather independent, quite stubborn, of strong altruistic feelings coming from within rather than from an externally imposed order.
She possessed a strong religious attitude along with childish guilt feelings and a need for expiation. Her feeling of guilt was not based on concrete experience, rather she had a general inclination to react with feeling of guilt; concrete events served as a trigger eliciting this feeling in her. She idealized phenomena and persons. She was impulsive, hotheaded, capable of opposing her parents; she demanded her own rights, and if denied cried or became stubborn.
Awakening of proper reflection in her was rather difficult in moments of strong emotional tension. Breaking of resistance was never applied, because when tried, the child’s emotional balance was all too soon visibly affected. One of her basic characteristics was a quick change in moods and an all too easy passing from laughter to tears and from tears back to laughter.
This girl represents definite traits of a cycloid type with considerable admixture of introversion. An ambivalent tendency to be older, on the one hand, and younger, even to be a baby, on the other. A definite need for positive regression, saturation with an atmosphere of fairy-tales, with heroic figures of fantasy, gnomes, movies, emotional richness and truthfulness.
Descriptive diagnosis may be briefly given as follows: a girl of cycloid type, of increased sensitivity in all main psychic areas. With a dynamic approach to everyday tasks, liable to suggestion, prone to psychic tensions with a tendency for explosion, interiorization, at times obsession. There is a tendency for regression, mainly positive. Definite nuclei of creative development with a need to subdue the environment to the needs of her own development.
274
Prognosis is good, assuming that an individual program of education and psychotherapy can be put into effect, with assistance for the growth of her creative forces and autopsychotherapy. Autopsychotherapy is possible even at such a young age. One introduces to some degree the dynamisms “subject-object in oneself,” dissatisfaction with oneself, perhaps even some light forms of the feeling of guilt, but above all certain ideal traits represented by persons whom the child desires to imitate. An authentic non-imitative personality ideal may develop later.
Therapeutic recommendation.
B.L. needs a wise, mildly pampering, and moderately sensitive atmosphere, help in positive regression with saturation with childish experiences. At the same time she needs a penetrating evaluation of her behavior. Decrease of her tension can be brought about through gradual strengthening of her ambition for reflection which she already had, but especially by directing her attention to greater independence from being excited by external stimuli by using her imagination, her memory and other inner resources. She also needs a considerable variety of occupations to meet her numerous interests and abilities.
A slow formation and development of a hierarchy of values should be encouraged leading to the development of her inner psychic milieu. In no case is the breaking of resistance advisable. She would benefit from short psychotherapeutic sessions in order to introduce dynamic insight into her understanding of herself and her relations with others. Under conditions of warmth and acceptance she may be more willing to improve her behavior on her own. She could then use her own judgment in the conflicts with her brother and sister.
A variety of sports and, games, and development of contacts with other children should be promoted.
Interpretation and discussion from the point of view of the theory of positive disintegration:
Two issues are of special importance here: positive regression with concomitant early development of self-control and help in the development of her inner psychic milieu.
275
Positive regression seems to be her great need. We saw her going back very often to the period of early childhood, very pleasant to her, even though she considered herself as especially lucky at the present time. She betrayed excessive need for cuddling, very strong need for a world of fantasy, dolls, etc. It was very appropriate that her parents considered these needs as natural and positive with the concomitant development, without exaggeration, of a sense of duty and responsibility by helping her mother, by special home assignments, by school work. This was being done without difficulty as the girl had an innate sense of duty combined with a need to help others.
With respect to the development of her inner milieu, it should be emphasized that this girl exhibited a definite tendency for hierarchization not only in the environment but in respect to herself as well. She had feelings of shame and guilt, and went through intense periods of wanting to improve her behavior and her school work. She was capable of self-control, even though she had an explosive temper. She also was showing a need for seeking, forming and strengthening her personal ideal with religious components. These traits indicated a need for a very refined approach in connection with the development of her inner milieu. At the same time her positive regression was expressed through childish fantasy, animism, and magical thinking. She wanted to be the younger child, she liked small children and often played with them. She also had inclination towards retrospection. She went through periods of rebellion, anger, maladjustment, and through periods of cooperation, syntony and sympathy.
(5) Case 21
The next case concerns R.R. a man 33 years old.
He was a scientist and a writer with mild obsessional tendency, with increased emotional and imaginational excitability, and undergoing multilevel disintegration.
In what follows we reproduce an excerpt from the third interview with the patient.
K.D.: You say that you are sick, that you have a psychoneu-
276
rosis and that you are afraid to develop a mental illness, is that correct?
R.R.: Yes, I am increasingly more concerned about my condition.
K.D.: Do you understand what is the cause of those fears in you? Are you afraid especially of that which is called “becoming mad”?
R.R.: Yes, that is what I fear. I am afraid to fall into a low level of self-awareness, of losing my human dignity.
K.D.: Can you say that you are presently losing that “humanity,” that your moral and intellectual forces are weakened, that your refinement is decreased, that you are becoming much less creative?
R.R.: (following reflection) No, I could not say that as yet, I do not notice such deterioration, but I see the increase in my fears, depression and obsession, weakness and chaos in my human contacts.
K.D.: Let us stop for a while to consider what you just said. Does it mean that your understanding of people has deteriorated, along with your capacity for sympathy and ability to help?
R.R.: No, it’s not that. What has been increased is the feeling of helplessness, feeling that my attitude of help for others meets with a vacuum, that I am incapable of helping them. However, I do feel their troubles, sadness, helplessness and often hopeless situation. I feel guilty of not being able to help.
K.D.: And your efficiency in work—is it being decreased, say during the last months in both quality and quantity?
R.R.: Yes, I thought so, but my colleagues say that I think and talk of issues in a more interesting manner during recent months, but that I work unevenly.
K.D.: Now, do you have some physical complaints, such as headaches, indigestion, sleeplessness?
R.R.: Yes. I sleep with difficulty, I have strange and depressing dreams. I often wake up with feelings of anxiety and headache. I often dream of animals, wildly and obsessively looking at me, terrible and yet unknown to me. I dream of grey walls, ditches; I flee before the unknown, become lost in unknown
277
cities. I am becoming dependent on some strange and unconnected situations. I felt as though deprived of will, condemned to unexplained activities directed by fate.
K.D.: Your dreams are characteristic for someone developing a higher level of consciousness, they appear oppressive, but in my opinion they are fully positive. Their content and climate are of the kind which Carl Jung called the “collective unconscious” expressed in “archetypes,” i.e. symbolized contents common to all men. There are there also your own individual contents but unconscious. You may want to study this and read some of Jung’s work on this subject. But now, tell me please, what are your most common experiences in life, what actually causes you anxiety at work, in your social life, in your family?
R.R.: I often feel psychic tension when dwelling on the objective valuelessness of all that which has for me, and my friends, a great subjective value. It seems like being captured in a poetic vision of that which is objective; I feel that objectivity is expressed by a deadly machine in the form of animosity and a brutal force exerted against subjectivity. But this kind of subjectivity, for us, is the highest type of reality, being destroyed, however, by mechanistic objectivity. I dwell on the possibility of losing my friends and close relatives, their smile, their presence, their aspirations, their unique personalities. It seems to me that reality is a tragic misunderstanding. I wake up at night to see all things in cruel realism. I notice the shamelessness and limitations in the thought and feeling, and the super-power of the so-called realists. I see the damage, injustice and humiliation of people who are spiritually strong but weak from the point of view of ability for adjustment to everyday life. I see around me death, as if waiting for me. I see the cowardly and nonsensical avoidance by people of essential issues. You understand and see, I am sure, doctor, that in all of which I am speaking there is much existential content. Yes, I have been fascinated for years with existential philosophy. But this is not for me an expression of a passing vogue or snobbery, or of my literary bent. It flows rather from my experiences and interests, which, as it were, went out to meet existential philosophy. I feel very strangely that our subjective
278
reality is something very essential for us, most essential indeed; that one must go through a rebellion of subjectivity against objectivity or reality, even if that rebellion is a priori condemned to failure.
I feel I must form a hierarchy of moral values, based on inner axiomatic imperatives, even if all those axioms and philosophy should be extinguished completely by death. There is something in those imperatives of subjective aspiration, which checks itself, which indicates its own way, which aspires at objectivity with conservation of individual values, which represents the need for continued being and development, because otherwise man becomes dehumanized.
That is why I am sick, doctor. Do you really think that there is a medicine for that?
K.D.: Now, did you not stop to think at times that you are not actually sick, but rather have something like a sixth sense, your increased sensitivity, psychic activity, concern for others and creative attitude towards reality? Do you not think that one must pay considerably for personal development or growth, especially if it be accelerated? Do you recall the expression of Korzecki in “Homeless People” when, speaking of himself, he says: “I have an over-educated consciousness”?
Do you not feel your own high responsibility for all that which happens among the people of your environment, closer and further, in your own milieu even if you don’t see the possibility of realizing your responsibility? That is normal, very normal, as it manifests the realization, to a high degree, of a “standard model norm.” No, you are not sick, you are very healthy mentally and you should not think that conditions of anxiety, of your excessive responsibility, protests, emotional attitude and actions against the so-called “normal life conditions,” feelings of dissatisfaction with yourself, are in any way pathological symptoms. On the contrary—it would be more pathological to adjust yourself excessively to a reality of a lower order. I don’t know if you would agree, but I believe that excessive adjustment to reality of a low level, excessive saturation with that reality, prohibits the cognition of reality of a higher type. One who is adjusted to all that
279
“which is,” irrespective of its values, has no possibility of creative power and will not adjust himself to that “which ought to be.”
R.R.: You are right—perhaps I should say I would think you are right—but that is hardly a normal psychiatric treatment, doctor. It seems that psychiatrists do not think as you do. On the basis of my experience I must say that to most of them my case is just like so many other cases-subject to pharmacological treatment, “treatment” which ignores the real problems but expects to accomplish everything by prescribing rest or sexual indulgence.
Furthermore, I feel lonely with my “pathological” experiences. I am very often alone because I do not want to burden my relatives with my own “fancies.” And so my life is passed in ambivalent attitudes between that which is close, worthy, really close, creative, between that which one should live through and digest and the need for fleeing from pain, misunderstanding, and human injustice. It seems that we have to build on ourselves, on our own deep humanistic criteria, and fulfill our obligations “to the end.” It may be that out of that “fear and trembling”—as Kierkegaard says—there will finally come real knowledge, discovery of the grain of truth, at present quite inaccessible to us, unexpected, and yet somehow foreseen in our very fight with adverse fate.
Interpretation of therapy from the point of view of positive disintegration.
We don’t deal here with a psychoneurosis as a sickness, but rather with the symptoms of the process of positive disintegration in its multilevel phase, with basic dynamisms of that phase such as disquietude, feelings of inferiority towards one-self, sense of guilt, feverish seeking of a disposing and directing center at a higher level and a personality ideal which would express the ability to feel the most universal needs of man, to have empathy towards those needs and aims.
The normal clinical diagnosis of anxiety psychoneurosis with existential traits gives us little to go on. The patient is in a condition of a very strong emotional tension with depressional
280
and anxiety components. The essential help for him is the confirmation of the conviction that his symptoms have elements of creative, positive psychic development.
Formation within the family milieu of conditions conducive to contact with nature, quiet, an artistic milieu, help in a proper attitude towards his work, and appreciation of his efforts, remain our fundamental directives.
(6) Case 22
Barbara was 17 years old. She had a very high, universal sensitivity especially with regard to affect and imagination. She was rebellious toward her parents, especially her mother. Barbara had a tendency towards neurotic playacting and superficial cynicism. Her emotional tensions and conflicts were easily transposed to the autonomic nervous system, causing headaches, accelerated heartbeat, menstrual disorders.
As a child she was well liked and caressed by her parents. She was brought up in an atmosphere of warmth and care given to an only daughter. She was growing up with tendencies for strong identification with her parents, especially her mother.
In the last two years there was a breakup of marriage, the fault of both parents. Barbara more or less knew about her parents' extramarital sexual relations. When her father left home, she stayed with her mother, with a strong protest towards both, but especially towards her mother.
This was her first interview with me.
K.D.: Shall I call you by your first name, or Miss?
Barbara: As you like, doctor (after some thought) I prefer my first name. But what is the reason for this attention in my case?
K.D.: I cannot say, Barbara, that this is a very kind opening on your part, but I have no bad feelings.
Barbara: What would you care to know about me, doctor?
K.D.: It is not the question of finding out something, the point is helping you.
Barbara: And how do you want to help me, doctor, is it in making me believe in lies on which I was being fed?
281
K.D.: No, certainly not, I want simply to help you by showing where you can separate truth from falsehood in the environment as well as in yourself.
Barbara: And how can you do it, if I don’t believe you? And, first of all, tell me please, do you have your own children whom you love and do you tell them the truth, or fables to be treated as truth? And—one thing more—do you have a wife whom you betray?
K.D.: Really, you don’t have much inhibition at this moment, but it’s all very well. You see, Barbara, I am at that age when one understands very many things—or nothing. I think, however, that at least I understand some. I have many faults, but those who know me have no doubt about one thing: my truthfulness. How can I prove to you that my family relations are not and will not be jeopardized? I would like to acquaint you, Barbara, with some of my friends, with whom I have had a close relationship for several years, you will be able then to talk to them and to verify all that I am telling you. You have considerable ability for observation and I can see it on the basis of my long experience. But do tell me please, why are you so keenly interested in the behavior of others; are you really so very suspicious? Is that what you feel most deeply in your heart, what causes you most concern?
Barbara: Yes, I feel deeply, and strongly (she becomes excited). I want to find out, I want to verify, that all this is a lie. Because even men of your age look at me with the special look and this repulses me. I mock that (more excitedly). I want to lie, too (very excitedly). I want to make love freely, betray and continuously play but have no concern, making it all very coldly; I want to be a good actress, and then to avenge, always avenge.
K.D.: But on whom, Barbara, and for what?
Barbara: On all, on everything, for making dirty all that which; I believed.
K.D.: Barbara you don’t have to believe me, but I believe you and I will tell you another thing, that I am beginning to respect you much for what you said. But on the other hand I know that your behavior must eventually depend more on:
282
yourself, on your own experience and conclusions, and less on the truth or falsehood of others, even closest relatives. Barbara: (Slowly becoming more quiet)—It is easy for you to say. I am sorry, doctor, for my improper way of behaving, but I think that all that is easy for you to say with your experience, but it’s much more difficult to accept for me. You see, I have my examples. It is true that all those whom we take as examples have two faces or sides, outer and inner, and is not the inner face worse and more dirty than the outer?
K.D.: Barbara, it is very difficult to convince you at this time. I don’t want to tell you much. Let me tell you this much; that I know personally a great many people, in whom the outer and inner picture harmonize in a very positive way.
Let me tell you only this much today, remember that I am trying to look at you from the inner side, from the side of your motives and your history, the side of your deep emotional movements. I do not care much what it is that you are saying in words. I would very much like to see you give voice to that in yourself which is so much offended, but so truly positive. That it may talk as your own, independent of the external environment, circumstances and momentary instinctual drives which are as determined as chemical reactions. I hope we shall meet again—and, if you will permit—perhaps more than once.
Interpretation of psychotherapy from the point of view of the theory of positive disintegration:
We are dealing here with a young girl of high sensitivity, emotional, psychomotor and imaginational excitability, with a tendency for violent reactions, periodic narrowing of reflection due to affective difficulties. Barbara has many positive traits, so important in development, such as spontaneity, sincerity, a certain natural integrity and dignity. She is prone to psychic breakdown, prone to acting on impulse and to narrowing of consciousness. She is given to some demonstrativeness. In medical language, she would be called hysterical. Of course, such clinical diagnosis tells us little.
The main therapeutic indications are, as we saw from the
283
excerpt of the interview, strengthening and development of her confidence in the positive sides of reality, rebuilding of her faith in moral standards, gradual decrease of tension, development of reflection, insight and practice in developing the dynamism “subject-object in oneself.” In that way, slowly, a disposing and directing center would be established at a higher level.
Through the strengthening of reflection and dynamic insight there should follow a slow emergence of some dynamisms of the inner psychic milieu with feelings of dissatisfaction with herself, inferiority with respect to her own unfulfilled potential, the dynamism “subject-object in oneself” and the third factor. It is important that the building of a disposing and directing center at a high level, with a personality ideal included, based on the grounds of a sincere need for moral standards, develop harmoniously with the formation of her inner psychic milieu and the deepening of multilevel disintegration.
It should be emphasized that Barbara at that time had not yet completely passed through unilevel disintegration and had already entered rather definitely into the stage of multilevel disintegration.
3. Comparison of Psychotherapeutic Programs
Let us try now to describe in some more detail the differences in psychotherapy of each one of these six cases, only to stress once more that the basis for differentiation of psychotherapy in each individual case are the differences in psychic overexcitability and differences in the stages of development (type of disintegration and the structure of the inner psychic milieu).
In case 17 (S. Mo.) we are dealing with the borderline of unilevel and multilevel disintegration. This together with S. Mo’s tetanoidal traits, with his obsessive perfectionism without a deeper understanding of the developmental sequence and hierarchy of self-perfection, makes it necessary to pay special attention to methods of relaxation as a tool in reducing his narrowly oriented tensions. It is necessary, therefore, to apply a systematic program of relaxation as a long-term
284
measure, and also to apply some short term relaxation treatments to deal with the immediate tensions.
In addition in all such cases when the patient in question is someone bright and creative it is most essential to carry-out a universal analysis of his creative potential. Proper use of creative interests and abilities reinforces healthy dynamisms of disintegration and promotes slow emergence of a disposing, and directing center at a higher level.
In cases 18 and 19 the thrust of therapy is directed to changing the environmental influence from a negative to a positive attitude. In case 18 this is the most important task of therapy.
In the case of the boy W. K. we are dealing with pre-pubertal age and a history of frustration which developed into a psychoneurosis of failure. Primary attention of therapy goes to work with the people in his family and his school environment. It is necessary to provide such conditions and such occasions that the boy could discover for himself that he is capable, that certain things he knows better how to do, that he can help others both intellectually and morally. The change of attitude in his environment to a positive understanding of his abilities, introvert sensitivity, and positive traits of his, character is a necessary part of providing him with an external support to facilitate the change of his negative self-concept to a positive one.
In Kristine’s case in contrast to the therapeutic strategy for W. K. and in part also to S. Mo.’s therapy, the main effort goes first to promote basic internal changes by stimulating her creative richness (childlike freshness, animism, fantasy, sensitivity to the feelings of others, insight). After this it is also necessary to change the attitude towards her of her family and her social environment by explaining to them the value of her creative abilities and that her infantilism and her “regression” are the natural source of her creativity.
In cases like Kristine’s, where we are dealing with a rich endowment for accelerated development, therapy is an occasion for providing the “patient” with enlightenment and confirmation as to the level already achieved and assistance toward
285
making it more of a stable base for further development. From this base one promotes then increasingly stronger prospection towards seeing and developing a global hierarchy of values and a personality ideal.
In case 20 (B. L.) we have to take into account that although the girl is only 10 years old she has great richness, many forms of psychic overexcitability and very strong psychic tensions. First aid, so to speak, is to so organize her environment as to reduce her tensions and give less occasion for their arousal. Thus partially freed she then could build up her own inner psychic milieu and mitigate its tensions. To start with it is necessary to help her develop her abilities yet without forcing anything that would lead to tension. If the girl switches her interests, even if she does it many times, this should be met with understanding, calmness and assistance in the pursuit of her newly elected fancy. She has to be given total support in the positive aspects of her needs to regress to earlier childhood.
This psychotherapeutic approach is not much different than the one described for the preceding case, except that in this case we are dealing with greater than Kristine’s “psychic imbalance” related to B. L.’s younger age, her greater obsessiveness and stubbornness.
Considering the advanced stage of multilevel disintegration of R. R. (Case 21) and his constellation of emotional, imaginational and intellectual overexcitability, psychotherapy has to take the direction of further expanding his perception of many levels of reality. R. R. needs assistance in a systematic elaboration of a program of succor to others in their “existential pains.” This would bring him to make his altruistic experiences more objective. One can expect that such work will bring greater calm to R.R. reducing to a large extent his tensions as yet too disunited and too little consciously organized.
On the basis of the analysis of his creative experiences one must convince R. R. that he is not only mentally healthy but that his growth is intense. He is coming slowly to a milder approach to his problems; at the same time his approach becomes deeper as he penetrates more into his personality ideal.
286
R. R.’s case is similar to the first (Case 17) but is more complex and developmentally more advanced.
In the last case (Barbara), we are dealing with multiple forms of overexcitability and a borderline of unilevel and multilevel disintegration, however the weight of disintegration is toward the multilevel. Barbara displays some hysterical traits, but of a fairly high level of functions, combined with strong aggressive and subconsciously controlled tendencies. Here psychotherapy needs to be based on methods of relaxation, on non-opposition to the client but rather on development of self-awareness, on stimulating the awakening of the dynamism “subject-object in oneself.” Barbara also needs help in learning to differentiate human types and levels of their development in order to attenuate her aggressiveness and give room to understanding and tolerance.
It is essential here that she makes use of her own creative abilities, and perhaps discovers in herself some new ones.
In this brief comparative rundown of psychotherapeutic strategies for each of the six presented cases we have tried not only to show the different types of disintegration and overexcitability but also in what way individual interests, abilities, and experiences are used as a means of promoting and supporting further growth.
287
288 (blank page)
GLOSSARY
ABDOMINAL REFLEX. Contraction of the muscles of the abdominal wall in response to stroking the overlying skin.
ABULIA. Loss of will; inability to decide on anything.
ACCELERATED DEVELOPMENT. Type of development characterized by multiple forms of psychic overexcitability (primarily emotional, imaginational, and intellectual), strong creative instinct, and strong autonomous factors. Accelerated development tends towards organized multilevel disintegration and secondary integration. It, thereby, tends towards transcending the psychological type and the biological life cycle. See Transcending the psychological type, Transcending the biological life cycle.
ADJUSTMENT. See Negative Adjustment, Positive Adjustment, Negative Maladjustment, and Positive Maladjustment.
AFFECTIVE PERSEVERATION. A tendency toward exploration and development of deep emotional relations and interests. It leads to few but very close relationships of love and friendship, or to a very profound dedication to one’s vocation. It occurs in individuals who are both emotional and introverted. They experience deeply and strongly, they remember their experiences vividly because of enhanced affective memory. Affective perseveration is related to the development of such attitudes as faithfulness to principles, loyalty in friendship, and constancy of interests. This quality is developmentally positive.
AMBIEQUAL TYPE. A type of personality differentiated by Rorschach which gives on the inkblot test a balance of response between internal movement and sensitivity to colors. It corresponds somewhat to the balance between introversion (emotional self-sufficiency and exclusivity, self-reference for norms and values), creativity, dependence on the external world, and sensitivity to it (need for emotional contact with environment, conformity with others, relative lack of self-reference).
AMBITENDENCIES. Contrary drives which are struggling for dominance yet never gaining it for an extended period of time. For example, greed and the accumulation of money may conflict
289
with the desire to spend it all and have a good time, a death wish (suicidal tendency) may conflict with the drive to self-preservation. As in Ambivalences these are conflicts between drives of the same level, therefore they are unilevel, and as such are characteristic of unilevel disintegration.
AMBIVALENCES. Conflicting attitudes as of obedience and rebellion, inferiority and superiority, love and hate, etc. Ambivalences are characteristic dynamisms of unilevel disintegration. The sense of higher and lower values is absent, the conflicting feelings are of equal value, therefore, they represent one and the same level.
AMPHOTONIA. See Autonomic Disequilibrium.
ANIMISM. The belief that objects in nature, or natural phenomena, are endowed with their own consciousness, or are inhabited by souls or spirits.
ARRHYTHMIA. A change in the rhythm or force of heartbeat. Arrhythmia may be caused by organic changes or by an alteration in the control of heartbeat without physical impairment (it is, therefore, a functional disorder).
ASTHENIA. Weakness, also tendency towards depression as in psychic asthenia (psychasthenia).
ASTHENIC. A type of body build characterized by small trunk and long limbs, also tending towards feelings of inferiority, weakness, passivity. Underestimates himself, is uncertain in his behavior and gives way.
ASTONISHMENT WITH ONESELF. The feeling that some of one’s mental qualities are surprising and unexpected. It is one of the earliest developmental dynamisms, and is mainly cognitive in nature, though not exclusively. It is active at the time of transition from unilevel to multilevel disintegration, usually accompanied by disquietude and dissatisfaction with oneself.
AUTHENTICITY, AUTHENTISM. Authenticity denotes a high degree of unity of one’s thinking, emotions, and activity. Authentism involves conscious activity in accordance with one’s “inner truth,” i.e. one’s autonomously developed hierarchy of values; it is a developmental force.
AUTISM, or AUTISTIC THINKING. Mental activity serving to gratify the thinker without respect to actual reality. Portrayed by Thurber in “The Secret Life of Walter Mitty.”
AUTOMATIC DYNAMISMS. Mental processes stemming from constitutional typological factors lacking conscious inner transformation, e.g. the “spontaneity” of action painting or “happenings.”
290
AUTONOMIC DISEQUILIBRIUM. Amphotonia, Dystonia, or Vagosympathetic Dystonia. Lack of balance between the activity of the sympathetic and the parasympathetic nervous systems, characterized by quick switches of dominance from one system to the other (see Autonomic Lability). Autonomic disequilibrium is characteristic of the lower neuroses.
AUTONOMIC DISORGANIZATION. The most evolved stage of Autonomic Disequilibrium (q.v.). It is expressed in the alternating strength of activity of the two autonomic systems: the sympathetic and the parasympathetic. It is observed as a prevalence of activity of the sympathetic nervous system in one field (e.g. digestive, or circulatory) and at the same time a prevalence of activity of the parasympathetic system in another field (e.g. genito-urinary, or respiratory).
AUTONOMIC LABILITY. A tendency to sudden transfer of tension between the sympathetic and the parasympathetic nervous systems. These reactions have disturbing consequences, as for instance, sudden drop of blood pressure and fainting spells, or the reverse when a sudden rise in blood pressure is spontaneously compensated by bleeding from the nose or mouth.
AUTONOMIC NERVOUS SYSTEM. A system of neurons controlling the involuntary activity of the viscera: digestive organs, heart, lungs, kidneys, glands, etc. It has two parts, the sympathetic and the parasympathetic. The stimulation of the sympathetic system mobilizes the organism by quickening respiration, heart rate, raising the blood pressure, etc. The action of the parasympathetic system is for the most part functionally reciprocal. The excitation of one system results in the inhibition of the functions controlled by the other, for instance, the increase of respiration and heart rate suspends digestion.
AUTONOMIC SOMATIZATION. The transformation of acute psychological tension into nervous somatic symptoms under the control of the autonomic nervous system. For instance, an increase in the pulse rate, blushing, or growing pale, growing tense, hysterical paralysis, etc., occur as a result of a severe emotional experience. The symptoms and syndromes may grow from very weak to very strong. It is believed that in autonomic somatization the disturbance is due more to the lability of the autonomic nervous system rather than to the intensity of psychological processes. Cf. Psychosomatization.
AUTONOMY. A dynamism of inner freedom. It signifies a consciously developed independence from lower drives and from the influences of the external environment.
291
AUTOPSYCHOTHERAPY. Psychotherapy, preventive measures, or changes in living conditions consciously applied to oneself in order to control possible mental disequilibrium.
BABINSKI REFLEX. Spreading of toes when the sole of the foot is scratched. A sign of pathology in the nervous system.
CATATONIC SCHIZOPHRENIA, or CATATONIA. Type of schizophrenia characterized by slowness of movements, or prolonged immobility, sometimes by muscular rigidity and inflexibility.
CHWOSTEK REFLEX. Local contraction of facial muscles in response to being struck by a mallet or to other stimulus.
COENESTHESIA. The totality of internal sensations by which one perceives one’s own body. Coenesthesia is increased when emotional processes are converted into the processes controlled by the autonomic nervous system, and vice versa, and are experienced as numbness, fornication, or internal oppression. Disturbances of coenesthesia take the form of vertigo, palpitation, nausea, etc. Marked coenesthesia is frequent at the stage of unilevel disintegration and may represent an initial phase toward control of the autonomic nervous system by the growing personality.
CONFABULATION. More or less unconscious creation of imaginary experiences, often in great detail, to cover up memory gaps or other lacks of own material.
CONTACT INTROVERSION. Introversion combined with conscious need for external contact. It results from the transformation of rigid introversion into a mixed introvertive-extrovertive type. It is an example of the transformation of a one-sided psychological type to a richer one less delimited by constitutional factors. Thus it represents an expression of the developmental potential. Contact introversion is connected with the dynamism and process “subject-object in oneself.”
CONVERSION. A mental mechanism by means of which an emotional reaction is expressed in an alteration of a function of the body, e.g. paralysis of a limb as an escape from a threatening or painful situation, or as an extreme affective identification with a paralyzed beloved person. Conversion reaction is characteristic of hysteria.
CREATIVE DYNAMISMS. Different abilities and talents finding their expression in a search for “otherness,” for non-stereotype facets of reality. All developmental dynamisms are creative by their power of transforming the individual and his perception of reality.
292
CREATIVE INSTINCT. An assembly of cohesively organized forces, often of great intensity, oriented toward a search for the new and the different in the external and the internal reality. Creative instinct is associated with accelerated development.
CUTANEOUS REFLEX. Wrinkling of the skin or gooseflesh upon mechanical stimulation of the skin.
CYCLOID. Refers to a person who shows relatively marked but normal swings of mood between excitement and depression, less strong than in the cyclothymic (q.v.).
CYCLOTHYMIC. Exhibiting alternating moods of elation and depression, activity and inactivity, with mood swings out of proportion to apparent stimuli. A mild form of manic-depressive behavior.
DEFENSE THROUGH DEVELOPMENT. With the progress of development the defensive (i.e. protective) forces localize themselves at a high level toward the service of individual growth. Mental development is the best protection against mental disorder. It is the lack of mental growth, or its stalemate, that favors mental illness.
DELUSIONAL CENTER. A disposing and directing center identified with a delusion (of persecution, jealousy, etc.) which controls behavior.
DERMOGRAPHIA. Sensitivity of the skin to local mechanical irritation. When pressed or scratched the skin produces a reddish, or sometimes white, raised mark which may stay for a short while or a long time, in which case we have a prolonged and more intense dermographic response.
DEVELOPMENTAL INSTINCT. The source of all mental developmental forces of the individual. It is absent in mental retardation and psychopathy.
DEVELOPMENTAL POTENTIAL. The constitutional endowment which determines the character and the extent of mental growth possible for a given individual. The developmental potential can be assessed on the basis of the following components: psychic overexcitability (q.v.), special abilities and talents, and autonomous factors (notably the Third factor).
DISINTEGRATION. Loosening, disorganization, or dissolution of mental structures and functions. See Unilevel Disintegration, Multilevel Disintegration, Negative Disintegration, and Positive Disintegration.
DISPOSING AND DIRECTING CENTER. A center which controls behavior over a short or long period of time. At a low level
293
of human development this center is identical with either one or a group of primitive drives (e.g. self-preservation, sexual, aggressive, etc.). At higher levels of development this center becomes an independent dynamism working towards harmonious unification of personality.
DISQUIETUDE WITH ONESELF. The feeling of uneasiness with oneself; one of the earliest dynamism marking the beginning of multilevel disintegration.
DISSATISFACTION WITH ONESELF, or Discontent with oneself. An early form of the dynamism of valuation (the third factor). A potent motivator of conscious development.
DRIVE. A concrete instinctive need of great intensity demanding satisfaction.
DYNAMIC INSIGHT, or “Prise de conscience.” Strong global momentary states of self-awareness. They tend to generate dynamic understanding of one’s behavior with the consequences of changing it.
DYNAMISM. Biological or mental force controlling behavior and its development. Instincts, drives, and intellectual processes combined with emotions are dynamisms.
DYSTONIA. See Autonomic Disequilibrium.
ECSTASY. Extreme absorption of attention resulting in a semi-trance as a consequence of intense contemplation of a limited field; a state characteristic of mystical experiences.
EKKLISIS. A term introduced by von Monakow to describe one of the two biopsychic vectors of behavioral patterns of living beings: approach and avoidance, attraction and repulsion, syntony and dislike, flight and aggression. Ekklisis is the name for the outward movement, Klisis is the name for the approach movement.
EMOTIONAL IMMATURITY. The persistence of emotional and intellectual qualities characteristic of children and youth past a young age. Associated with tendencies to Positive Regression (q.v.) it is an essential component of creative development.
EMOTIONAL RETARDATION. A negative form of Emotional Immaturity; lack of emotional development characterized by primitiveness and rigidity of affect, very low level of syntony and emotional sensitivity. Associated with psychopathy and some forms of mental retardation.
EMPATHY. High level of Syntony (q.v.).
ERYTHEMA PUDICUM. The tendency to blush because of feelings of shame, timidity, or inhibition. An indicator of emotional
294
overexcitability. It is often due to periodic heightened sensitivity to the opinions and judgments expressed by others. It is combined with somatopsychic sensitivity.
EVOLUTION. A development which proceeds from lower to higher levels of organization. Positive disintegration is the type of process through which individual human evolution occurs. See Involution.
EXISTENTIAL ANXIETY. Anxiety states on a very high level of development involving the awareness of the fact of one’s existence and the responsibility that follows from it. Fear for others prevails over fear for oneself. Existential anxiety arises on the basis of psychic overexcitability (q.v.) of alterocentric nature. It embraces empathic and intellectual components on a very wide range with the emphasis on the human dilemma of existential choice. It is also related to the awareness of the universality of human experience as expressed by St. Paul: “If anyone is weak, do I not share this weakness? If anyone is made to stumble, does not my heart blaze with indignation?” (II Cor. 11, 29).
EXISTENTIAL HYSTERIA. A psychoneurosis at a high level of development arising on a background of existential experiences and actions prompted by empathy (alterocentric preoccupations). With hysteria it has the following similarities, though expressed at a higher level: intense affects, strong dramatization, attitude of gesture, demonstrativeness, tendency toward ecstasy or contemplation.
EXISTENTIAL PSYCHONEUROSIS. Psychoneurosis on a high level of development which involves a dominance of existential preoccupations. These existential components are peculiar to each kind of psychoneurosis-depressive, anxiety, infantile, obsessive, etc.
EXTRAVERT. A type of personality exhibiting strong interest in external reality, inclined to rely in his judgments and experiences on the opinions of his environment; inclined to syntony and adaptation to others, does not tolerate solitude.
FLEXIBILITAS CEREA. See Waxy Flexibility.
FUNCTIONS. The instruments of mental and emotional equipment, e.g. reality function, empathy, identification, responsibility, intuition. See Levels of Functions.
HEBEPHRENIC SCHIZOPHRENIA, or Hebephrenia. Type of schizophrenia characterized by shallow inappropriate affects, unpredictable behavior, silly mannerisms.
HIERARCHIZATION. The process of developing or activating different emotional levels. It stems from conflicts of value
295
which reflect the existence of feelings corresponding to higher and lower values (i.e. more preferred vs. lens preferred choices). A hierarchy of values is a hierarchy of higher and lower levels of emotions.
HYPERKINESIS. Excessive restlessness of movements.
HYPERTONIA, or Autonomic Hypertonia. High tension of the Autonomic nervous system (q.v.).
HYPOBULIA. Lowered ability to act or to make decisions. Less severe than Abulia.
HYPOMANIC. Refers to mild manic conditions, characterized by restlessness, flight of ideas, distraction.
HYPOTONIA, or Autonomic Hypotonia. Low tension of the Autonomic nervous system (q.v.).
INFANTILISM. A combination of infantile mental qualities. In its positive form it is associated with plasticity and emotional sincerity characteristic of children. In its negative form it is associated with general lack of developmental potential as in mental retardation.
INFERIORITY TOWARD ONESELF. The feeling consisting in the experiencing and awareness of the disparity between the level at which one is and the higher one toward which one strives. It is the shock of realization of one’s unfaithfulness to the ideal of personality, to the hierarchy of values which begins to take shape but as yet lack stability, followed by a desire and actions to transform oneself.
INHIBITION. Means of control of physiological or mental processes at any level of activity by reducing or stopping the flow of a given process
INNER PSYCHIC MILIEU, or internal mental environment. The totality of mental dynamisms of a low or high degree of consciousness. The inner psychic milieu may be hierarchical, as in multilevel disintegration, or ahierarchical, as in unilevel disintegration. The inner psychic milieu as a ground for positive development must be hierarchical, and it is this type which is normally understood under the term.
INNER PSYCHIC TRANSFORMATION. The process by which the work of developmental change in man’s mental structure is carried out. It makes possible the transcending of the psychological type and of the biological life cycle (see Transcending).
INTEGRATION. Consists in an organization of instinctive, emotional and intellectual functions into a coordinated structure. See Primitive Integration and Secondary Integration.
296
INTERNEUROTIC LEVELS. Psychoneurotic syndromes characteristic of different levels of development. For example, phobias, organ neuroses and hypochondria are limited to Level II (unilevel disintegration), while paranoid and catatonic schizophrenias can occur at Level II and III and thus are disorders of higher level representing greater complexity and greater possibility of growth. Psychoneurotic anxiety and depression are still higher because they do not occur below Level III (see Table II, p, 110). Correct and precise diagnosis of a syndrome helps to identify the developmental level of a patient.
INTRANEUROTIC LEVELS. Levels of functions differentiated within the same psychoneurotic syndrome. Lower levels are characterized by predominant somatic control while higher levels by predominant mental control. For example within the category of psychasthenias neurasthenia represents a higher level than hypochondria, but lower level than psychasthenia, all three involving the same group of functions (see Table III, p. 113).
INTROVERT. A type of personality having difficult contact with his environment, inclined to base his behavior on his own judgment, imagination and experience; inclined to solitude, avoids other especially at times of grave difficulties.
INVOLUTION. Negative development. Opposite of evolution (q.v.). Development which proceeds from higher to a lower level of organization. It tends toward severe disorders (psychosis, psychopathy, mental retardation), and may lead to the dissolution of mental organization.
KINAESTHESIS. The sense of movement derived from receptors in skeletal muscles, joints, etc. In the Rorschach—a movement response.
KLISIS. A term introduced by van Monakow to describe the approach tendency as one of the two main behavioral vectors. See Ekklisis.
LEVEL I. Primitive integration (q.v.).
LEVEL II. Unilevel disintegration (q.v.). LEVEL III. Spontaneous multilevel disintegration (q.v.).
LEVEL IV. Organized multilevel disintegration (q.v.).
LEVEL V. Secondary integration (q.v.).
LEVELS OF FUNCTIONS. The qualitative and quantitative differences which appear in mental functions as a result of developmental changes. Lower levels of functions are characterized by automatism, impulsiveness, stereotypy, egocentrism, lack or low degree of consciousness. Higher levels of functions
297
show distinct consciousness, inner psychic transformation, autonomousness, creativity.
LABILITY, see Autonomic Lability.
MAGICAL THINKING. An emotional, imaginational, and intuitive type of thinking based on the assumption (most often unconscious) that some phenomena may operate exempt from the causality of the laws of nature. Magical thinking explains different phenomena in a miraculous or fantastic way.
MEDITATION. Practice of mental concentration leading to inner calmness and sense of well-being.
MEDITATIVE EMPATHY. An expression of sympathy towards another person but with strong reflective, and even meditative, components. It is a high level of syntony of closely integrated intellectual elements. The intellectual elements do not diminish such empathy but rather enrich and develop it: “I know you and I always refine this knowledge; yet this does not diminish my feeling for you but differentiates it.”
MENTAL HEALTH. Development towards higher levels of mental functions, towards the discovery and realization of higher cognitive, moral, social, and aesthetic values and their organization into a hierarchy in accordance with one’s own authentic personality ideal.
MENTAL ILLNESS. The absence or deficiency of processes which effect the development of emotional and instinctive functions. It takes the form of either (1) a strongly integrated, primitive, psychopathic structure, or (2) a negative, nondevelopmental disintegration which may end in dissolution of mental structures and functions.
MIGRATORY NEUROSIS. An organ neurosis with a tendency to periodical quick migration from affecting the function of one organ to affecting another, or from one system of organs to another.
MULTILEVEL DISINTEGRATION. Multilevel disintegration is a process of developing an authentic hierarchy of values from conflicts between higher and lower levels of instinctive, emotional and intellectual functions. The conflicts are conscious since they involve the awareness of valuing one level over another, therefore, they are conflicts of value.
MULTILEVELNESS. Division of functions into different levels, for instance, the spinal, subcortical, and cortical levels in the nervous system. Individual perception of many levels of external and internal reality appears at a certain stage of development, here called multilevel disintegration. See Levels of Functions.
298
NEGATIVE. Adevelopmental, involutional. Refers to factors which arrest development or act against it either by making mental organization rigid, or discomposing it (involution).
NEGATIVE ADJUSTMENT. Nondevelopmental adjustment. Unqualified conformity to a hierarchy of values prevailing in a person’s social environment. The values are accepted without an independent critical evaluation. It is an acceptance of an external system of values without autonomous choice. An adjustment to “what is.”
NEGATIVE DEVELOPMENTAL POTENTIAL. Constitutional predisposition to psychosis, psychopathy, or mental retardation, or other severe disorders preventing development or leading to the dissolution of mental life.
NEGATIVE DISINTEGRATION, or involutional disintegration. A process characterized by the operation of dynamisms dissolving the organization of mental structures and functions. Its end is chronic mental illness. It occurs almost exclusively at the stage of unilevel disintegration.
NEGATIVE MALADJUSTMENT. Rejection of social norms and accepted patterns of behavior because of the controlling power of primitive drives and nondevelopmental or pathologically deformed structures and functions. In the extreme case it takes the form of psychosis, psychopathy, or criminal activity.
NEGATIVE REGRESSION. Thinking, experiencing, and acting resulting from regression to lower and more primitive levels of behavior.
NERVOUSNESS. Enhanced psychic overexcitability in the form of excitability of movements, senses, affect, imagination, and intellect. Nervousness does not in any way entail the impairment of mental functions.
NEURASTHENIA. A type of psychoneurosis characterized by cycles of excitation followed by excessive fatigue, even exhaustion. Lower level of psychasthenia, frequently associated with obsessions and phobias.
NEUROPSYCHIC PROCESSES. Mental and emotional processes occurring at the neurological level intimately connected with somatic functions and primitive emotional and instinctual functions.
NEUROSIS. Psychophysiological or psychosomatic disorders characterized by a dominance of somatic processes. There are no detectable organic defects, although the functions may be severely affected.
299
NUCLEI. Incipient forms of developmental factors which may or may not develop.
OCULOCARDIAC REFLEX. Reflex obtained by lightly pressing on the eyeballs (closed eyelids) and measuring the pulse. The reflex is said to be positive if fluctuation in the pulse rate is observed.
ONE-SIDED DEVELOPMENT. Type of development limited to one talent or ability, or to a narrow range of abilities and mental functions. In such development the creative instinct and empathy appear absent. In exceptionally capable individuals their one sided development may come under the control of a primitive disposing and directing center and in the extreme case may take the form of psychopathy or paranoia.
ORGANIZED MULTILEVEL DISINTEGRATION. Developmental level IV. A stage of development when a high level of self-awareness makes possible a greater degree of self-direction and self-determination. External conflicts disappear, and internal conflicts become less overwhelming and intense.
OVEREXCITABILITY. See Psychic Overexcitability.
PARANOID SCHIZOPHRENIA. Type of schizophrenia characterized by delusions of persecution, or delusions of power, or both.
PARASYMPATHETIC NERVOUS SYSTEM. See Autonomic nervous system.
PARTIAL DISINTEGRATION. Disintegration within, one or a few related dynamisms. It may lead either to reintegration at a previous level, to reintegration at a lower level (primitive integration), to partial integration at a higher level, or to global disintegration. Partial disintegrations followed by partial integrations at a higher level characterize the developmental pattern of people with average developmental potential. In contrast, global disintegration and global secondary integration (if any) are the privilege of people with rich endowment for accelerated development.
PARTIAL SECONDARY INTEGRATION. A cohesive organization of some of the emotional and instinctive functions at a higher level. It comes about as a result of partial multilevel disintegration.
PATHOLOGICAL HEREDITARY ENDOWMENT. The occurrence in the family tree of psychoses, psychopathy, mental retardation, or other forms of mental disorder.
PATHOLOGICAL RUMINATION. A type of obsession characterized by the tendency to dwell on the same problem without seeking
300
to find a solution to break the “vicious circle.” It is typical of unilevel processes of disintegration.
PERSEVERATION. Persistent and recurrent thought or image; compulsive repetition of the same phrase or word over and over again. See also Affective Perseveration.
PERSONALITY. A self-aware, self-chosen, self-affirmed, and self-determined unity of essential individual psychic qualities. Personality as defined here appears at the level of secondary-integration (q.v.).
PERSONALITY IDEAL. An individual standard against which one evaluates one’s actual personality structure. It arises out of one’s experience and development. At first the ideal may be an imitation, nevertheless, with the growth of individual awareness it becomes authentic and autonomous to eventually become the highest dynamism in the development of personality.
PERVERSION NEUROSIS. A neurosis resulting from a very strong attraction and repulsion and internal conflict in relation to uncommon sexual urges such as fetishism, necrophilia, homosexuality, or severe masturbation. Internal tension and self-awareness are acting strongly and simultaneously, because there is the awareness of the strength of the impulses and their aberrant nature together with a refinement which removes the possibility of hurting or shocking a sexual partner.
POLARITY. Existing between two opposites, as in emotional fluctuations between pleasant and unpleasant, between joyous and sad.
POSITIVE. Developmental or evolutional. Also used to refer to development with emerging direction of growth from lower to a higher level of functions (process of hierarchization).
POSITIVE ADJUSTMENT, or developmental adjustment. Conformity to higher levels of a hierarchy of values self-discovered and consciously followed. It is an acceptance of values after critical examination and an autonomous choice. It is an adjustment to “what ought to be.” Such hierarchy of values is controlled by (or developed from) the personality ideal.
POSITIVE DISINTEGRATION. A process of development involving characteristic dynamisms and some degree of awareness of development. It releases the creative powers of the individual, it enriches his psyche, and it carries his growth toward a higher level of psychological functioning.
There are four stages of positive disintegration forming an invariant sequence: (1) unilevel disintegration, (2) spontaneous multilevel disintegration, (3) organized multilevel disintegration, (4) transition to secondary integration.
301
POSITIVE MALADJUSTMENT. A conflict with and rejection of those standards and attitudes of one’s social environment which are incompatible with one’s growing awareness of a higher scale of values which is developing as an internal imperative.
POSITIVE REGRESSION. Regression in the service of the ego. Temporary regression to an earlier emotional period, or withdrawal from current activities in search of isolation. It is caused by a need for saturation with the carefree and warm experiences of childhood, or by a need to have psychic rest, or a time off to accommodate an experiential load. Positive regression allows an individual to prepare more fully the unfolding of his creative potential, to prevent mental disorders, to preserve and develop his autonomy. It is common in people with emotional and imaginational overexcitability.
PRESPASM. A prespasmatic state. A state of “preparation” for psychic spasm (q.v.) resulting from painful external or internal stimuli and tension. These stimuli evoke unpleasant reactions and result in fear or flight (avoidance) in acute, unconscious forms.
PREVENTIVE MECHANISMS. See Protective Mechanisms.
PRIMITIVE DRIVES. Drives (q.v.) operating at the level of primitive integration. Their action is characterized by great intensity, inflexibility, automatism, egocentrism, biological control. They lack the conscious components of reflection, empathy, inhibition. For instance, sexual drive at the primitive level precludes personal involvement with the sexual partner, precludes considerations of discomfort or hurt sustained by the partner.
PRIMITIVE FUNCTIONS. Emotional and instinctive functions (q.v.) operating at the level of primitive integration. They are characterized by automatism, impulsiveness, stereotypy, egocentrism, lack of inhibition, lack or low degree of consciousness.
PRIMITIVE INTEGRATION, or Primary Integration. Developmental level I. An integration of all mental functions into a cohesive structure controlled by primitive drives.
PRISE DE CONSCIENCE. See Dynamic Insight.
PROSPECTION. An ability to temporarily transpose one’s thoughts and feelings into the future, usually associated with rich imagination and fantasy. It may also have a strong intuitive component as a sense of timing of the development to come. Characterizes not only dreamers but also dynamic individuals given to construction of hypotheses or long-range planning.
302
PROTECTIVE MECHANISMS. Psychoneurotic processes and dynamisms which by their relatively mild disintegrating power protect against mental breakdown or suicide. The richer the hereditary endowment the stronger are the protective dynamisms. Cf. Defense through development.
PSYCHASTHENIA. A type of psychoneurosis characterized by lowered biopsychic tonus, especially in regard to primitive functions and adjustment to actual reality. Psychasthenia is characterized by feelings of inadequacy, obsessions, anxieties (especially existential), depressions.
PSYCHIC OVEREXCITABILITY. Higher than average responsiveness to stimuli, manifested either by psychomotor, sensual, emotional (affective), imaginational, or intellectual excitability, or the combination thereof.
PSYCHIC SPASM. Psychic state analogous to a physiological spasm. It is the sudden arrest in an unpleasant way of ongoing mental activity as a result of new and unfamiliar experiences. It may also be evoked by the sudden appearance of an uncontrollable impulse.
PSYCHIC SPASMOPHILIA. Condition analogous to the “spasmophilic” constitution (see Spasmophilia). Psychic spasmophilia does not depend on the physical spasmophilic constitution but may, when present, function together with it. The characteristic traits are excessive sudden responses to positive and negative psychic stimuli. Psychic spasmophilia is an expression of susceptibility to frustration or to being hurt. It acts also as a psychic defense against too strong stimuli by giving a warning signal to consciousness about impending emotional danger or overwhelming joy, which may upset the balance. This mechanism serves the role of delaying or “diluting” negative and positive stimuli of an intensity higher than the system can handle.
PSYCHOMOTOR CRISIS. Acting out of psychic tension through temper tantrums, destructive behavior, running away, or hysterical conversion. Psychomotor crises are frequent in cases of psychomotor and emotional overexcitability not combined with other enriching components of the developmental potential which in this case is rather limited, and due to the absence of a multilevel inner psychic milieu does not offer the possibility of a positive release.
PSYCHONEUROSIS. A more or less organized form of growth through positive disintegration. Lower psychoneuroses are predominantly psychosomatic in nature, higher psychoneuroses are highly conscious internal struggles whose tensions and frustrations are not anymore translated into somatic disorders.
303
PSYCHOSOMATIZATION. An excessive tendency for transposition of intense psychical experiences onto somatic processes. The high tension is absorbed by somatic functions thereby altering their course. This can be manifested as paresis, paralysis, hysterical numbness, etc. In psychosomatization the genesis of a disturbance is believed to be in the psyche. Cf. Autonomic Somatization.
REALITY FUNCTION. A function which guides the behavior of the individual in his testing of internal and external reality. It adapts his behavior to the demands of those levels of reality which he perceives as the more vital. Reality function at a low level deals with the basic needs of everyday living. Reality function at a high, level deals with the experiences and processes of inner creative reality.
REGRESSION. See Negative Regression and Positive Regression.
SCHIZONEUROSIS. A psychopathological syndrome on the borderline of psychoneurosis and schizophrenia (psychosis).
SCHIZOPHRENIA SIMPLEX. Type of schizophrenia characterized by withdrawal, apathy, indifference. It progresses slowly but irreversibly.
SCHIZOTHYMIC. Showing tendency to an uneven, diffuse, inconsistent behavior with weak syntony and poor adjustment to the environment, often with symptoms of queerness.
SECONDARY INTEGRATION. Developmental level V. The integration of all mental functions into a harmonious structure controlled by higher emotions such as the dynamism of personality ideal, autonomy and authenticity. Secondary integration is the outcome of the full process of positive disintegration.
SELF-PERFECTION INSTINCT. The higher form of the creative instinct (q.v.). It appears in accelerated development when the individual’s primary concern is his self-growth.
SIMPLE SCHIZOPHRENIA. See Schizophrenia Simplex.
SOMATOPSYCHIC. Refers to the lowest level of psychoneurotic processes, i.e. those occurring without any participation of consciousness. At the somatopsychic level mental processes are almost entirely under the control of biological processes. The next higher level is the psychosomatic where psychological tensions are transposed to somatic processes via the autonomic nervous system.
SOMNAMBULISM. Sleepwalking. Walking and carrying out complex activities while in sleep, or a hypnotic or related state..
SPASMOPHILIA. The tendency toward muscular twitching, spasms, or convulsions from even slight mechanical or electrical stimula-
304
tion. Psychic Spasmophilia (q.v.) is a metaphor used here to describe easily mobilized strong and sudden involuntary emotional reactions, tensions, which are experienced not unlike internal convulsions.
SPONTANEOUS MULTILEVEL DISINTEGRATION. Developmental Level III. The stage of development which occurs with the emergence of a direction of development and a sense of “higher” and “lower.” These two phenomena are strictly inter-dependent. They are the result of intense emotional experiences and spontaneously developing conflicts of value (see Hierarchization).
“STUTTERING” OF SOMATIC FUNCTIONS. A tendency toward spastic psychophysical activity. It is observed as sudden blushing or growing pale, as pharyngeal spasms, or “stuttering” of urination. It is the manifestation of the transformation of very strong somatopsychic (q.v.) tension to spastic symptoms.
SUBJECT-OBJECT IN ONESELF. One of the main developmental dynamisms which consists in observing one’s own mental life in an attempt to better understand oneself and to evaluate oneself critically. It is a process of looking at oneself as if from outside (the self as object) and of perceiving the individuality of others (the other as subject, i.e. individual knower).
SYMPATHETIC NERVOUS SYSTEM. See Autonomic nervous system.
SYMPATHIGOTONIA. A state resulting from high tension in the sympathetic nervous system manifested by accelerated pulse, high blood pressure, dilated pupils, or hypoacidity of the stomach.
SYNTONY. Responsiveness to the environment, chiming in with. Primitive syntony is impulsive behavior and is not much different from gregariousness. Higher levels of syntony involve insight into other people’s feelings and experiences. More conscious and deliberate forms of syntony combined with an attitude of helpfulness we call empathy.
TETANOIDAL PERSONALITY. Personality type differentiated by Jaensch and characterized by muscular twitching, spasms, tendency to convulsions, etc., as in tetany. The activity of the parasympathetic nervous system is prevalent. Psychologically a tetanoidal individual shows somewhat uncoordinated behavior; his responses are not harmonized and are not integrated.
THIRD FACTOR. The autonomous factor of development. The first factor is the constitutional endowment, the second factor
305
is the social environment. The third factor is the dynamism of conscious choice (valuation) by which one affirms or rejects certain qualities in oneself and in one’s environment.
TRANSCENDENTAL OBSESSION. Obsession with problems of transcendence, i.e. with problems of supersensory reality. It is not much different from a scientist’s obsession with an unsolved problem, or an artist’s obsession with the search for new means of expression.
TRANSCENDING THE BIOLOGICAL LIFE CYCLE. Replacement of somatic determinants of maturation, aging, or disease, by mental determinants of rich psychic development (accelerated development), continued creativity in spite of aging, continued psychic growth past maturity, etc.
TRANSCENDING THE PSYCHOLOGICAL TYPE. Introduction of traits of opposite type to one’s original type, e.g. an extravert becoming to some extent an introvert. This developmental change occurs as a consequence of the dynamism of inner psychic transformation and is characteristic of accelerated development.
UNILEVEL DISINTEGRATION. Developmental Level II. Protracted and recurrent conflicts between drives and emotional states of similar level and of similar intensity appearing as ambivalences and ambitendencies (q.v.), e.g. changing and alternating states of attraction and repulsion, love and hate, joy and sadness, excitement and depression, moodiness. The conflicts may not be consciously experienced. When they are they are experienced as pulls of equal value, in contrast to multilevel conflicts, and, therefore, do not tend towards a solution but seek immediate palliatives like alcohol, drugs, or suicide.
VAGOSYMPATHETIC DYSTONIA. See Autonomic Disequilibrium.
VAGOSYMPATHETIC SYSTEM. See Autonomic Nervous System.
VAGOTONIA. Excessive excitability of the vagus nerve. A state resulting from high tension in the vagus nerve manifested by slowing down of pulse, arrhythmia, low blood pressure, constricted pupils, peripheral vascular disorders.
VALUE. See Hierarchization.
WAXY FLEXIBILITY. A passive response by which a person’s arm or posture retains the position in which it has been placed. Usually thought to be characteristic of catatonic schizophrenia this response is easily obtained from normal individuals.
306
BIBLIOGRAPHY
Abély, P. De quelques equivoques psychiatriques . Annales medico-psychologiques, 117, 46-78, 1959.
Abély, P., and M. Delaville . Nouvelles recherches cliniques et biologiques sur les syndromes discordantes. Paris: Masson et Cie, 1960.
Adler, A. Study of organ inferiority and its psychical compensation. New York: Nervous and Mental Diseases Publishing Co., 1917.
Adler, A. Understanding human nature. New York: Greenberg, 1927.
Adler, A. Individualpsychologie in der schule. Leipzig: Deuticke, 1924.
Adler, A. Problems of neurosis, a book of case histories. New York: Cosmopolitan Book Corp., 1930.
Adler, A. A social interest, a challenge to mankind. London: Faber and Faber, Ltd., 1938.
Albérès, R. M. Miguel de Unamuno. Paris: Presses Universitaires. 1957.
Albérès, R. M., and P. de Boisdeferre. Franz Kafka: the torment of man. New York: Philosophical Library, 1968.
Bleuler, E. Die psychoanalyse Freuds. Wien: Deuticke, 1911.
Bleuler, M. Krankheits verlauf, persdnlichkeit and verwandschaft schizophrenir and ihre gegenseitigen beziehungen. Leipzig, Thieme, 1941.
Brun, R. Allgemeine neurosenlehre. 3 auflage, Basel: Benno Schwabe, 1954.
Campbell, C. M. Towards mental health. The schizophrenic process. Cambridge: Harvard University Press, 1933.
Corrie, J., and C. G. Jung. Psychologie im abriss. Zurich: Rascher and Co., 1928.
Dąbrowski, K. Psychological bases of self-mutilation . Genetic Psychology Monographs, 19, 1-104, 1937.
Dąbrowski, K. Pojecie zdrowia psychicznego (The concept of mental health). Zdrowie Psychiczne, 2, 37-51, 1947.
307
Dąbrowski, K. Nerwowość dzieci I mlodziezy (The nervousness of children and youth). Warsaw: Panstwowe Zaklady Wydawnictw Szkolnych, 1958.
Dąbrowski, K. Spoleczno-wychowawcza psychiatria dziecieca. (Socio-educational child psychiatry). Warsaw: Panstwowe Zaklady Wydawnictw Szkolnych, 1959.
Dąbrowski, K. Remarques sur la typologie basee sur la theorie de la desintegration positive . Annales medico-psychologiques, 118 (2), 401-406, 1960.
Dąbrowski, K. Principes, structures et dynamismes du milieu psychique interne. A Crianca Portuguesa, 21, 507-535, 1963.
Dąbrowski, K. Psychonerwice (Psychoneuroses). Postepy Higieny I Medycyny Doświadczalnej, 17, 305-345, 1963.
Dąbrowski, K. 0 dezyntegracji pozytywnej. Warsaw: Panstwowe Zaklady Wydawnictw Lekarskich, 1964a.
Dąbrowski, K. Positive disintegration. Boston: Little, Brown and Co., 1964b.
Dąbrowski, K. Prophylaxie des nevroses infantiles ou prophylaxie par les nevroses infantiles? Proceedings of the Fourth World Congress of Psychiatry, vol. 1, 127-130. Madrid, September, 1966. Amsterdam: Excerpta Medica Foundation.
Dąbrowski, K. Interneurotic and intraneurotic differences in levels of functions. Proceedings of the Fourth World Congress of Psychiatry, vol. 2, 2876-2878. Madrid, September, 1966. Amsterdam: Excerpta Medica Foundation.
Dąbrowski, K. The theory of positive disintegration. International Journal of Psychiatry, 2, 229-244, 1966.
Dąbrowski, K. La decompentation des structures psychonevrotiques d'apres la theorie de la desintegration positive. Annales medico-psychologiques, 125 (2), 475-482, 1967a.
Dąbrowski, K. Personality-shaping through positive disintegration. Boston: Little, Brown, and Co., 1967b.
Dąbrowski, K. Le milieu psychique interne. Annales medico-psychologiques, 126(2), 457-485, 1968.
Dąbrowski, K. Multilevelness of emotional and instinctive functions. University of Alberta, Edmonton, Alberta, 1970.
Dąbrowski, K., A. Kawczak, and M. M. Piechowski. Mental growth through positive disintegration. London: Gryf Publications Ltd., 1970.
Dąbrowski, K., and M. M. Piechowski. Les emotions superieures et l'objectivite d'evaluation . Annales medico-psychologiques, 127 (2), 589-613, 1969.
308
Dawid, J. W . Ostatnie mysli I wyznania (Last thoughts and confessions). Warsaw: Nasza Ksiggarnia, 1935.
Erikson, E . Childhood and society. New York: W. W. Norton and Co., 1950.
Erikson, E . Identity and the life cycle. New York: International Universities Press, 1959.
Ey, H., and J. Rouart. Essai d'application des principes de Jackson a une conception dynamique de la neuropsychiatrie. Paris: Doin et Cie, 1938.
Frankl, V. E. Psychotherapy and existentialism; selected papers on logotherapy . New York: Washington Square Press, 1967.
Freud, S. Uber psychoanalyse. Wien: Deuticke, 1924.
Freud, S. A general introduction to psychoanalysis. Garden City, N.Y.: Garden City Publishing Co., 1943.
Freud, S. An outline of psychoanalysis. New York: W. W. Norton and Co., 1949.
Greenblatt, M., and H. C. Solomon, (Eds.). Frontal lobes and schizophrenia. New York: Springer, 1953.
Horney, K . The neurotic personality of our time. New York: W. W. Norton and Co., 1937.
Horney, K. Neurosis and human growth: the struggle toward self-realization. New York: W. W. Norton and Co., 1950.
Jackson, J. H. Selected writings. J. Taylor, ed. New York: Basic Books, 1958.
Jaensch, E. R. über den aufbau der wahrnehmungswelt and ihre struktur im jugendaltern. Leipzig: 1923.
Janet, P. Irene. In G. Murphy (Ed.) An outline of abnormal psychology. New York: The Modern Library, 1929.
Janet, P. Les neuroses. Paris: Flammarion, 1926.
Janet, P. The major symptoms of hysteria. New York: Macmillan Co., 1920.
Jones, E. Treatment of the neuroses. New York: W. Wood, 1920.
Jung, C. G. Psychologische typen. Zurich: Rascher and Co., 1921. (p, 483).
Jung, C. G. Das unbewusste in normalen and kranken seelenleben. Zurich: Rancher and Co., 1926. (p. 30).
Jung, C. G. Analytische psychology and erziehung. Heidelberg: Kampmann Verlag, 1928. (pp. 42 and 46).
Jung, C. G. Psychological reflections. New York: Harper Torch books, 1961.
Kretschmer, E. Physique and character; an investigation of the nature of constitution and of the theory of temperament. New
309
York: International Library of Psychology, Philosophy, and Scientific Method, 1925.
Kretschmer, E. The psychology of men of genius. New York International Library of Psychology, Philosophy, and the Scientific Method, 1931.
Kretschmer, E. Hysteria, reflex, and instinct. New York: Philosophical Library, 1960.
Laing, R. D. The divided self. London: Tavistock Publications, 1960,
Leighton, D. C. The distribution of psychiatric symptoms is a small town, Amer. J. of Psychiatry 112, 716-723, 1956.
Lindemann, E. Psycho-social factor: as stressor agents. In J. M. Tanner (Ed.), Stress and psychiatric disorders. Oxford: Blackwell Scientific Publications, 1960.
Lindemann, E., and D. Klein. Preventive intervention in individual and family crisis situations. In G. Caplan (Ed.), Prevention of mental disorders in children; initial exploration. New York: Basic Books, 1961.
Malcolm, N. Ludwig Wittengstein, a memoir with a biographical sketch by Georg Henrik von Wright. London, New York: Oxford University Press, 1958.
Maslow, A. H. Toward a psychology of being. New York: Van Nostrand, 1962.
Maslow, A, H. The psychology of science. New York: Harper and Row, 1966.
Masserman, J. H. Behavior and neurosis: an experimental psychoanalytic approach to psychobiological principles. Chicago: The University of Chicago Press, 1943.
Maudsley, H. The physiology and pathology of mind. London: Macmillan, 1868.
Maudsley, H. Body and mind. London: Macmillan, 1873.
May, R. Existential psychology. New York: Random House, 1961.
Mazurkewicz, J. Wstep do psychofizjologii normalnej (An introduction to normal psycholophysiology), Warsaw: PZWL, 1950.
Menninger, K. A., and J. L. Menninger. Love against hate. New York: Harcourt, Brace, and World, 1942.
Menninger, K. A., M. Mayham, and P. Pryyser. The vital balance: life process in mental health and illness. New York: The Viking Press, 1963.
Meyer, A. In A, Lief (Ed.), The commonsense psychiatry of Dr. Adolph Meyer: fifty-two selected papers edited with a biographical narrative by Alfred Lief. New York: McGraw-Hill, 1948.
310
Monakow, von C., and R. Mourgue. Introduction biologique a l'etude de la psychopathologie. Paris: Alcan, 1928.
Mowrer, 0. H. Crisis in psychiatry and religion. Princeton: Van Nostrand, 1961.
Mowrer, 0. H. The new group therapy. Princeton: Van Nostrand, 1964.
Mowrer, 0. H. Morality and mental health. Chicago: Rand McNally, 1967.
Nachmannsohn, M. Die hauptstroemungen der psychotherapy der gegenwart. Zurich: Rascher and Co., 1933 (p, 233).
Pavlov, I. P. Conditioned reflexes and psychiatry. New York: International Publishers, 1941.
Piotrowski, Z. Perceptanalysis; a fundamentally reworked, expanded and systematized Rorschach method. New York: Macmillan, 1957.
Richer, J. Girard de Nerval. Paris: Pierre Sechers Editions, 1962.
Rogers, C. R. Client-centered therapy, its current practice, implications, and theory. Boston: Houghton Mifflin, 1951.
Rogers, C. D. Therapy, personality, and interpersonal relationship in psychology. In Sigmund Koch (Ed.) Psychology: study of a science. New York: McGraw-Hill, 1959.
Rogers, C. R. Toward a modern approach to values; the valuing process in the mature person. J. of Abnormal and Social Psychology. 68, 160-167, 1964.
Rogers, C. R., and R. F. Dymond. (Ed.), Psychotherapy and personality change. Chicago: The University of Chicago Press, 1954.
Sargent, W. W., and E. Slater. An introduction to physical methods of treatment in psychiatry. Edinburgh: Livingstone, 1954.
Schultz, J. H., and W. Luthe. Autogenic training: a psychophysiologic approach in psychotherapy. New York: Grune and Stratton, 1959.
Seager, A. The glass house. The life of Theodore Roethke. New York: McGraw-Hill, 1968.
Sherrington, C. S. The integrative action of the nervous system. New Haven: Yale University Press, 1961.
Srole, L., T. S. Lagner, S. T. Michael, M. K. Opler, and T. A. C. Rennie. Mental health in the metropolis: the midtown Manhattan study. New York: McGraw-Hill, 1962.
Thomas, A. Les phenomenes de repercussivite. Paris: Masson et Cie, 1929.
311
Wallace, R. K. Physiological effects of transcendental meditation. Science. 167, 1751-1754, 1970.
Weininger, 0. über die letzten dienge. Vienna: Deuticke, 1926.
Wolpe, J. Psychotherapy by reciprocal inhibition. Stanford: Stanford University Press, 1958.
Zajaczkowski, H. Psychoterapeutyczne zwiazanie uczuciowe (Psycho-therapeutic emotional binds). Zdrowie psychiczne. 1, 34-43, 1961.
312
{{Back Cover}}
MENTAL GROWTH THROUGH POSITIVE DISINTEGRATION
“I consider this to be one of the most important contributions to psychological and psychiatric theory in this whole decade. There is little question in my mind that this book will be read for another decade or two, and very widely. It digs very deep and comes up with extremely important conclusions that will certainly change the course of psychological theorizing and the practice of psychotherapy for some time to come.”
Abraham H. Maslow
Brandeis University
PERSONALITY SHAPING THROUGH POSITIVE DISINTEGRATION
“Dr. Kazimierz Dąbrowski is no ordinary psychiatrist. Although educated as a physician, he has developed a conception of man and his “existential” vagaries which radically transcends the physical and biological realms; and although later trained in Freudian psychoanalysis, he has a point of view which, instead of denigrating morality and idealism, puts them in a place of supreme importance.
“Dr Dąbrowski has certainly been a pioneer in the development of the kind of psychiatry that is set forth in this book, and he deserves great credit for his originality and courage. But, at the same time there is nothing singular or eccentric about his particular orientation. It is, in fact, part and parcel of a widespread and growing perspective in clinical psychology and psychiatry which can only be described as revolutionary.”
O. Hobart Mowrer
University of Illinois
POSITIVE DISINTEGRATION
“Dąbrowski’s theory is not only interesting but even exciting in its breadth and depth if its implications. The ubiquity of psychological symptoms has always confounded a simple descriptive psycho-pathological approach to mental illness. Dąbrowski’s theory gives these symptoms a role in normal personality development that is consistent with their broad distribution as shown by epidemiological studies and as felt by those aware of the problems in themselves and in those around them.”
Jason Aronson
Harvard Medical School.

![]()